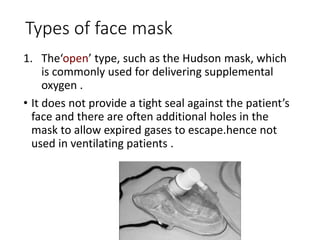
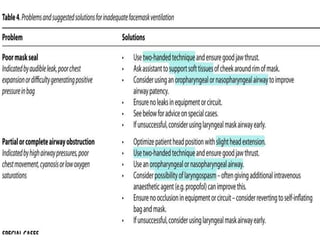
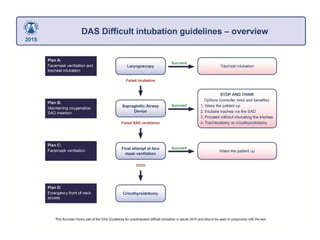
This document discusses techniques of mask ventilation. It begins by introducing mask ventilation as a noninvasive airway management technique used for short anesthetics or as a bridge to a more definitive airway. It then describes the types of face masks, including open masks for oxygen delivery and closed masks for ventilation. It discusses the parts of masks including the connector and harness. The document outlines techniques for mask application, including one-handed and two-handed techniques. It describes signs of inadequate mask ventilation and complications of mask ventilation such as skin allergy, nerve injury, gastric inflation, and eye or skin injuries. Throughout, it provides details on positioning, types of masks, application techniques, and complications to summarize techniques of mask ventilation.