Downloaded 24 times

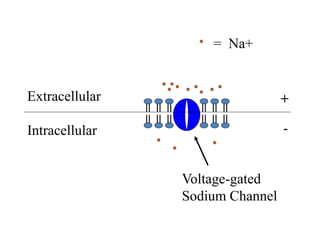
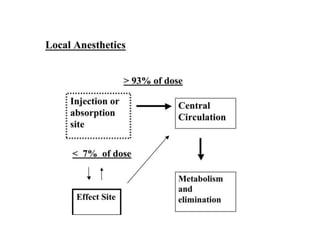

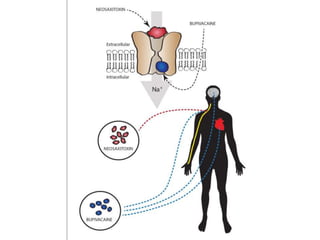
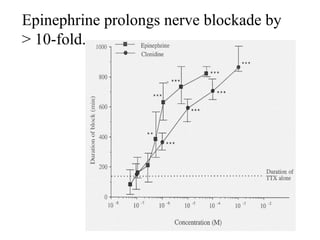
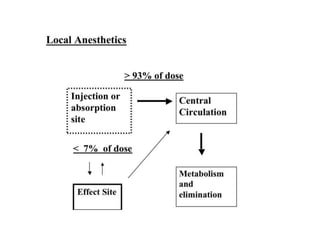
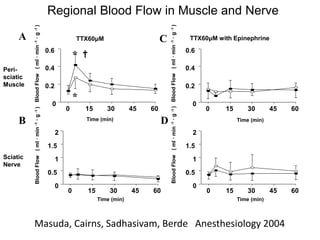
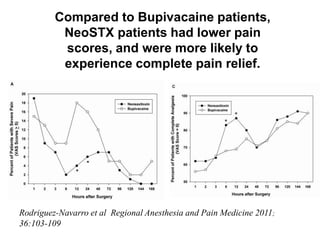
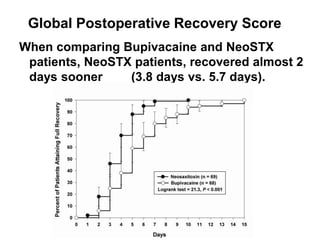

The lecture discusses the advantages and limitations of existing local anesthetics and the potential impact of new long-acting anesthetics like neosaxitoxin on clinical practice. Current local anesthetics often have short durations and systemic toxicity risks, while new developments, such as the use of liposomal formulations and site-1 sodium channel blockers, aim to enhance efficacy and safety. Neosaxitoxin shows promise in improving postoperative pain relief and recovery times, warranting continued research and development efforts.















































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)




![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)
