Downloaded 60 times
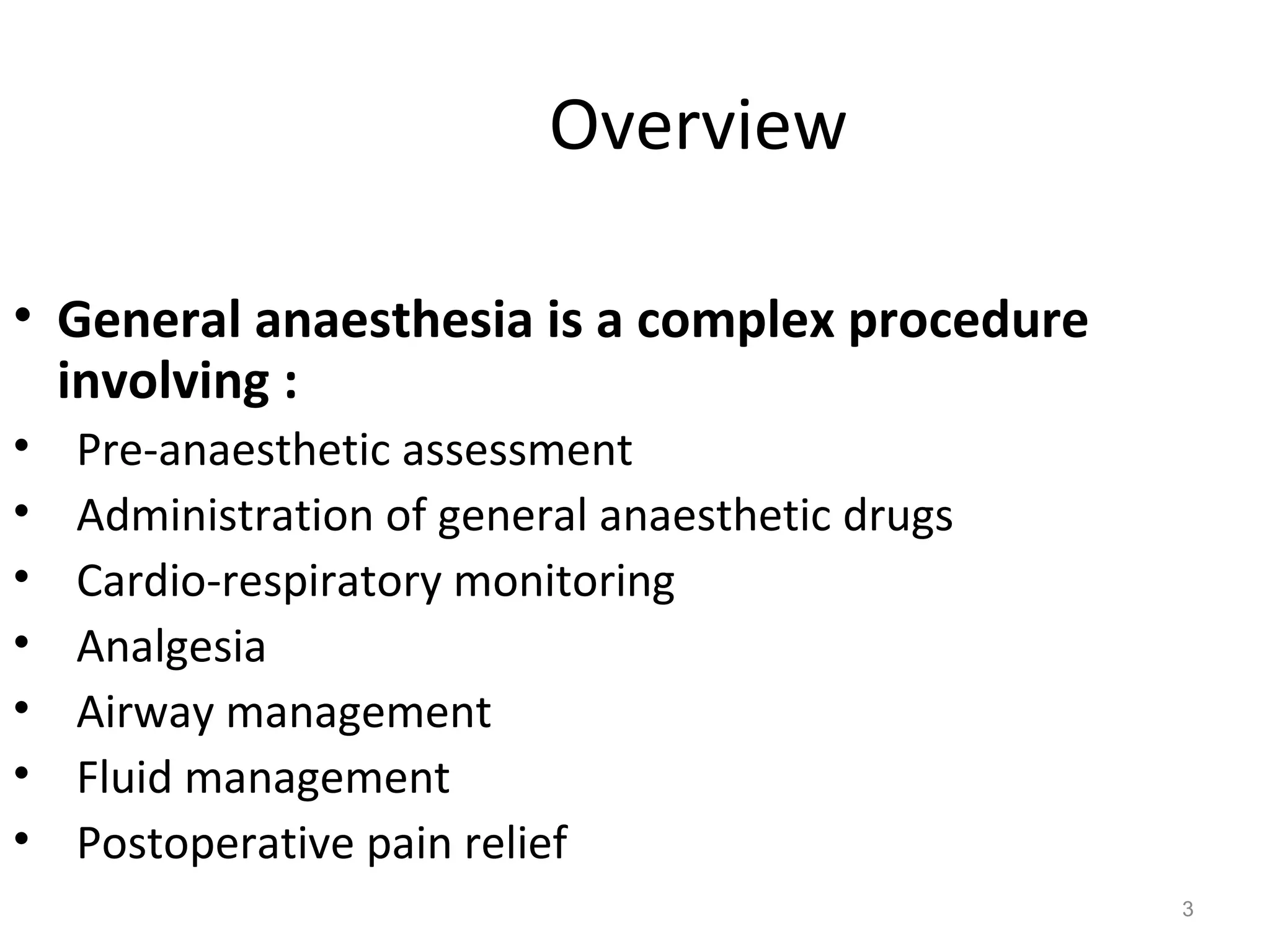



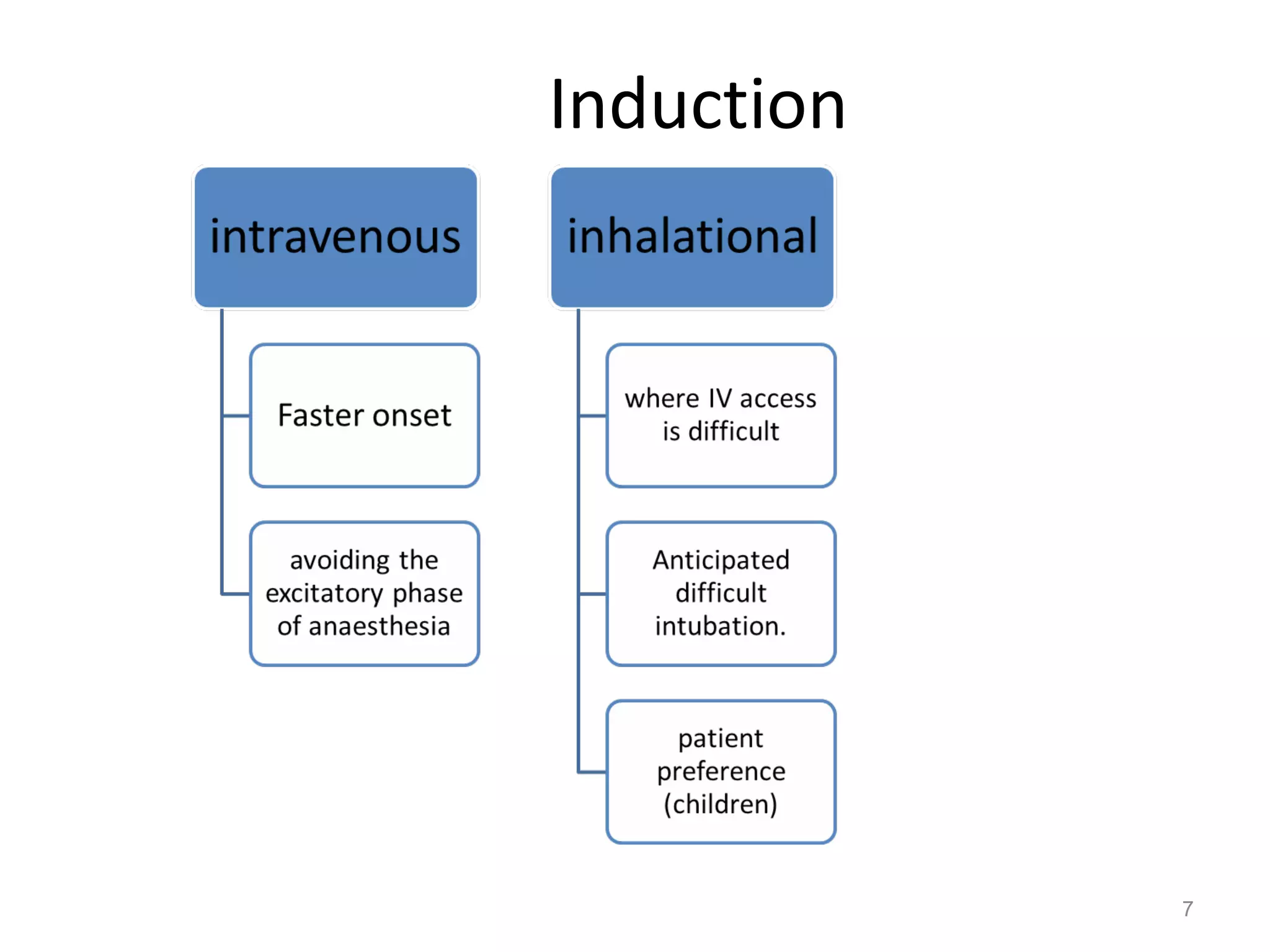













This document provides an overview of general anaesthesia, including: - It involves pre-anaesthetic assessment, administration of anaesthetic drugs, cardio-respiratory monitoring, analgesia, airway management, and fluid management. - Common intravenous induction agents are propofol, sodium thiopental, and ketamine which modulate GABA transmission. - Inhalational induction options include sevoflurane which causes less irritation. - Maintenance involves inhalation of oxygen, nitrous oxide, and volatile anaesthetic along with intravenous opioids. Total intravenous anaesthesia uses propofol infusion. - Airway management often uses endotracheal tubes or laryngeal masks. Monitoring includes ECG, pulse ox



































































