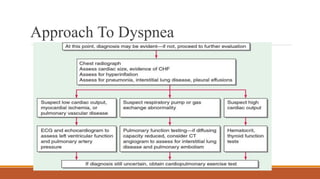
Approach to dyspnea
andcase discussions
Dr. Shubham Agarwal, JR (Med)
Dr. Sarada, SR (Med)
Faculty Preceptor- Prof. Sanjeev Sinha
3.
Loading…
What is Dyspnea?
•Dyspnea is the unusual and uncomfortable awareness of difficult or labored
breathing
• Normal resting patients are unaware of the act of breathing
• It is subjective and its quality is unique
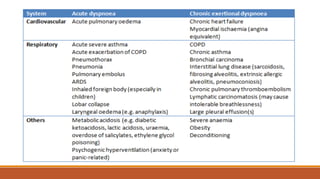
• ~ 95% of cases are due to one of five major causes: cardiac (e.g., CHF),
pulmonary (e.g., COPD, asthma, ILD), psychogenic factors, GERD, and
deconditioning
• Dyspnea is termed acute if it develops over hours to days and chronic when it
occurs for more than four to eight weeks.
4.
Some Distinct Terms
Orthopnea:
Dyspneaupon lying in the supine position. Characteristic of CHF and, in rare
cases, of bilateral diaphragmatic paralysis
Trepopnea:
Dyspnea upon lying in the lateral decubitus position. Most often occurs in
patients with CHF
Platypnea:
Dyspnea upon assuming the upright position
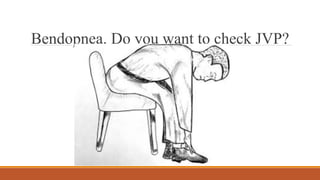
Bendopnea:
Dyspnea when leaning forward
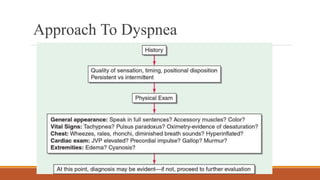
History In ACase Of Dyspnea
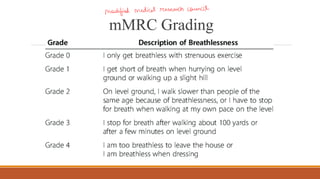
• Duration, onset, course and progression
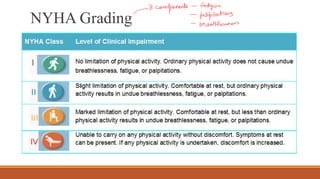
• Grade
• Associated symptoms: Substernal chest pain with myocardial ischemia; fever, cough, and sputum
with respiratory infections
• Positional variation of dyspnea (othopnea, platypnea, trepopnea) or PND
• Seasonal and diurnal variation: Intermittent dyspnea in asthma and COPD
• Smoking and environmental exposure history
• Tuberculosis: Past history/contact history/family history
• Socio-economic status
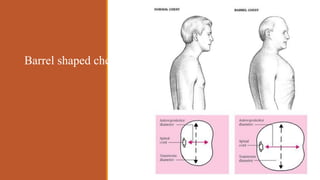
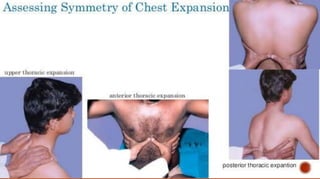
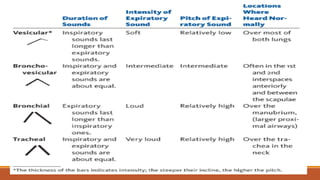
Respiratory System Examination
INSPECTION-
•Shape of the chest and movement of the chest (symmetry?)
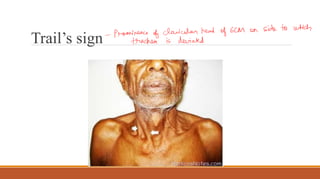
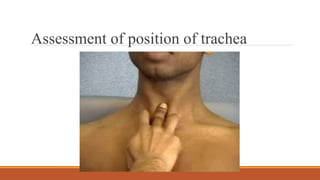
• Position of trachea
• Position of apical impulse
• Chest deformities, use of accessory muscles, dilated veins, scars or sinuses, indrawing of
intercostal spaces, visible fullness
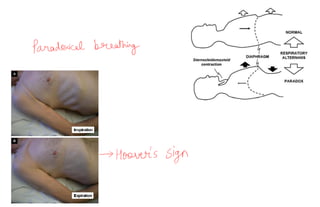
• Paradoxical breathing
• Lower chest indrawing (Hoover’s sign)
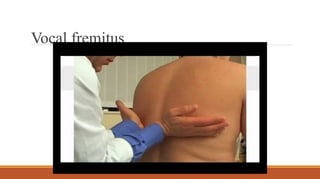
PALPATION-
• Any localrise of temperature or tenderness
• Confirming the findings of inspection
• Vocal fremitus
• Measurements: AP diameter, transverse diameter, chest circumference, hemithorax
measurements, expansion
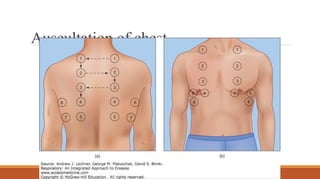
Respiratory System Examination
Loading…
HISTORY
I am presentingthe clinical case of Mr. J.B.S.
who is a 25 year old gentleman, works as a
truck-driver and hails from Ghimana,
Haryana.
He is brought by his brother and history was
obtained from the patient as well as the brother
and history seems to be reliable and adequate.
31.
CHIEF COMPLAINTS
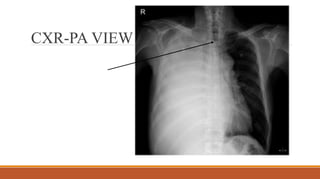
1. Feverfor the past 10 days
2. Right sided chest pain for the past 5 days
3. Shortness of breath for the past 3 days
32.
HOPI
The patient wasapparently asymptomatic 10 days back when he developed:
◦ Fever
◦ Low grade
◦ Undocumented
◦ Daily
◦ More pronounced in the evening
◦ Intermittent; Responded to OTC anti-pyretics
◦ A/w Loss of appetite, nigh sweats and generalized weakness
◦ Not a/w chills and rigor
◦ No h/o headache/ sore throat/ ear pain/ pain abdomen/ skin rash/ joint pain/ photosensitivity/
myalgias/ burning micturition/ loose stools/ leg pain
33.
Right sided chestpain:
• Sudden onset, severe
• Sharp, stabbing type of pain
• Describes it as a “catch in his breath” with deep breathing and coughing
• No radiation, referral or shifting of pain
• Decreased on lying to the right side
34.
Shortness of breath:
◦Acute in onset
◦ Present throughout the day (non-episodic)
◦ Gradually progressive over the past 3 days
◦ mMRC grade II -> III
◦ Associated with dry cough and right sided chest pain
◦ No postural/ diurnal variation
◦ No h/o palpitations/ orthopnea/ PND/ lower limb swelling
◦ No h/o worsening on exposure to dust/ pollen
35.
PAST HISTORY
No pasthistory of similar complaints in the past
No past history of any hospitalization or major surgical procedure
H/o TB contact (father is on ATT, diagnosed as Pulmonary TB 4 months back)
FAMILY HISTORY
No history of similar complaints in any of the family members
36.
PERSONAL-SOCIAL HISTORY
He worksas a rickshaw puller and resides in a pucca house. He has a family of seven people
with three people sharing one room. They have access to personal water supply and have a
separate washroom. They come under lower-middle class as per the Modified Kuppuswamy
scale.
He has normal bladder-bowel habits.
He complaints of reduced sleep over the past 5 days due to his physical symptoms.
He does not smoke or drink alcohol.
He is a strict vegetarian and reports loss of appetite over the past 10 days.
37.
GENERAL PHYSICAL
EXAMINATION
He isconscious, coherent, co-operative, alert and well
oriented to time, place and person
Decubitus- Prefers to lie on right lateral decubitus.
He has mild pallor.
No icterus/ cyanosis/ clubbing/ peripheral
lymphadenopathy/ pedal edema
Head to toe examination was unremarkable otherwise
38.
VITALS:
◦ PR- 110/min,Regular, good volume, no abnormal character, all peripheral pulses palpable, No
R-R or R-F delay
◦ BP- 110/70 mmHg in right arm in supine position
◦ RR-26/min, Regular, abdomino-thoracic, regular. Accessory muscle of respiration are
working.
◦ sPo2- 94% on Room air
◦ Temp- 101 F measured per-axillary at 04:00 PM
INSPECTION
●Upper Respiratory tract-WNL
●RR- 26/min, regular, abdomino-thoracic. Accessory muscles of respiration are working
●Fullness of intercostal spaces on the right side seen
●Reduced movement of the right side of the chest
●Apex impulse appears to be lateral to mid-clavicular line
●No swelling/ scars/ sinuses/ dilated veins on the chest wall
●No chest/ spine deformity noted
PALPATION
●No local riseof temperature
●No tenderness
●Trachea- shifted to the left side
●Apex beat- in 9th ICS, 1.5 cm lateral to MCL
●Chest wall expansion- Reduced on the right side
●Tactile Vocal Fremitus- Reduced on the right side
43.
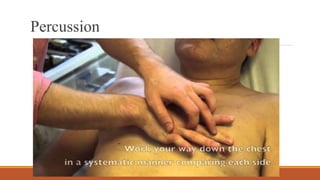
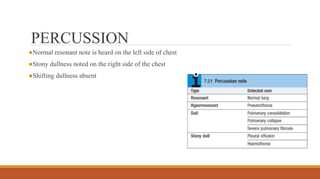
PERCUSSION
●Normal resonant noteis heard on the left side of chest
●Stony dullness noted on the right side of the chest
●Shifting dullness absent
SYSTEMIC EXAMINATION (contd..)
●Cardiovascularsystem- S1 S2 heard. No murmurs discernible
●CNS- Full GCS. No Focal neurological deficit.
●P/A- Soft, non tender. No organomegaly. Bowel sounds present.
46.
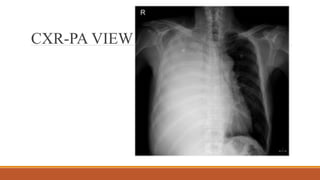
SUMMARY
➢25 year old,previously healthy male
➢Fever+ Pleuritic chest pain+ Shortness of breath
➢Tachypneic
➢Reduced movements on right side
➢Tracheal shift to left + Apex shifted laterally= Mediatinal shift to left
➢Stony dullness on right side
➢ Air entry absent on the right side
A 62-year-old manis referred by his GP to a respiratory outpatient clinic,
with a history of cough, sputum production and breathlessness. He has
had a persistent cough for the past 12 years and produces a teaspoonful of
mucopurulent phlegm on a daily basis. The breathlessness started 10
years previously and has progressively worsened, such that he is now
breathless on climbing 12 stairs at a normal pace. He has no nocturnal
chest symptoms and has received one course of antibiotics from his GP in
the last year. He is a current smoker and has a 44-pack year history. He
used to work in the demolition industry but took voluntary retirement at
the age of 55.
68.
DDx (based onhistory)
1. COPD
2. ILD (pneumoconiosis/asbestosis)
3. Bronchiectasis (but has smaller amount of sputum And no recurrent lung infections)
4. Concomitant heart failure
69.
O/E
The patient isbreathless on exertion but there is no cyanosis. He has
obvious finger clubbing. Respiratory rate is 22 breaths/min, blood pressure
is 160/90 mmHg, heart rate is regular at 96 beats/min and oxygen
saturations are 94% breathing room air. His jugular venous pulse (JVP) is
not elevated. Chest expansion and percussion are normal, but there are
mid- to late fine inspiratory crackles on chest auscultation. Both heart
sounds are normal and there is no peripheral oedema.
70.
Based on examinationand history now,
Findings are not typical of COPD (COPD – reduced lung expansion, on percussion –
hyperesonance, on auscultation – reduced lung sounds)
Mid inspiratory crackles are typical of lung fibrosis. So, In view of his occupation, most likely it is
pulmonary fibrosis – due to asbestos exposure.
71.
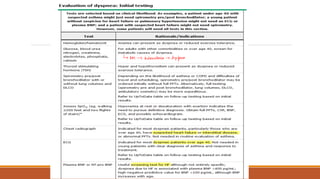
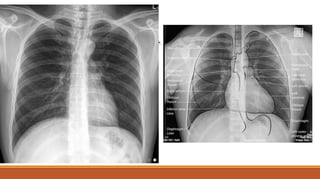
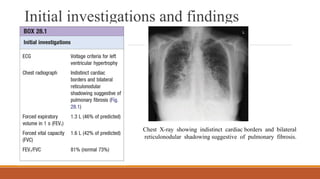
Initial investigations andfindings
Chest X-ray showing indistinct cardiac borders and bilateral
reticulonodular shadowing suggestive of pulmonary fibrosis.
72.
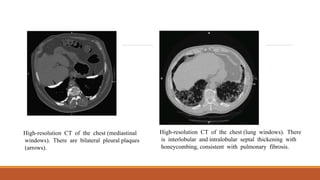
High-resolution CT ofthe chest (mediastinal
windows). There are bilateral pleural plaques
(arrows).
High-resolution CT of the chest (lung windows). There
is interlobular and intralobular septal thickening with
honeycombing, consistent with pulmonary fibrosis.