Downloaded 519 times
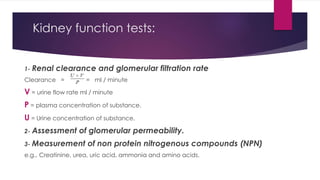
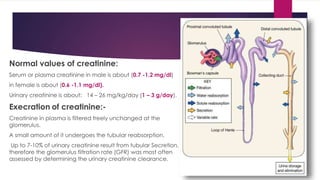
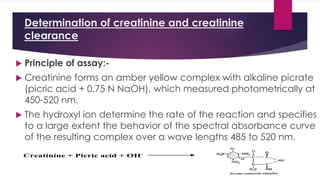
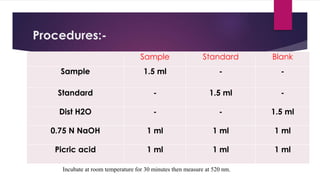
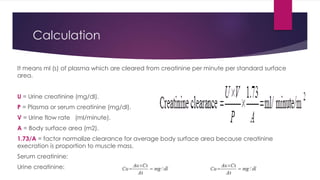

This document discusses creatinine and creatinine clearance as measures of kidney function. It describes how creatinine is produced in the body and excreted by the kidneys, and how measuring levels of creatinine in the blood and urine can provide information about glomerular filtration rate and kidney health. Specifically, creatinine clearance can be used as an indicator of glomerular filtration rate, since creatinine is produced at a constant rate and freely filtered by the kidneys. Both high and low levels of blood creatinine can indicate kidney abnormalities. The document also outlines the procedure for determining creatinine levels in samples.