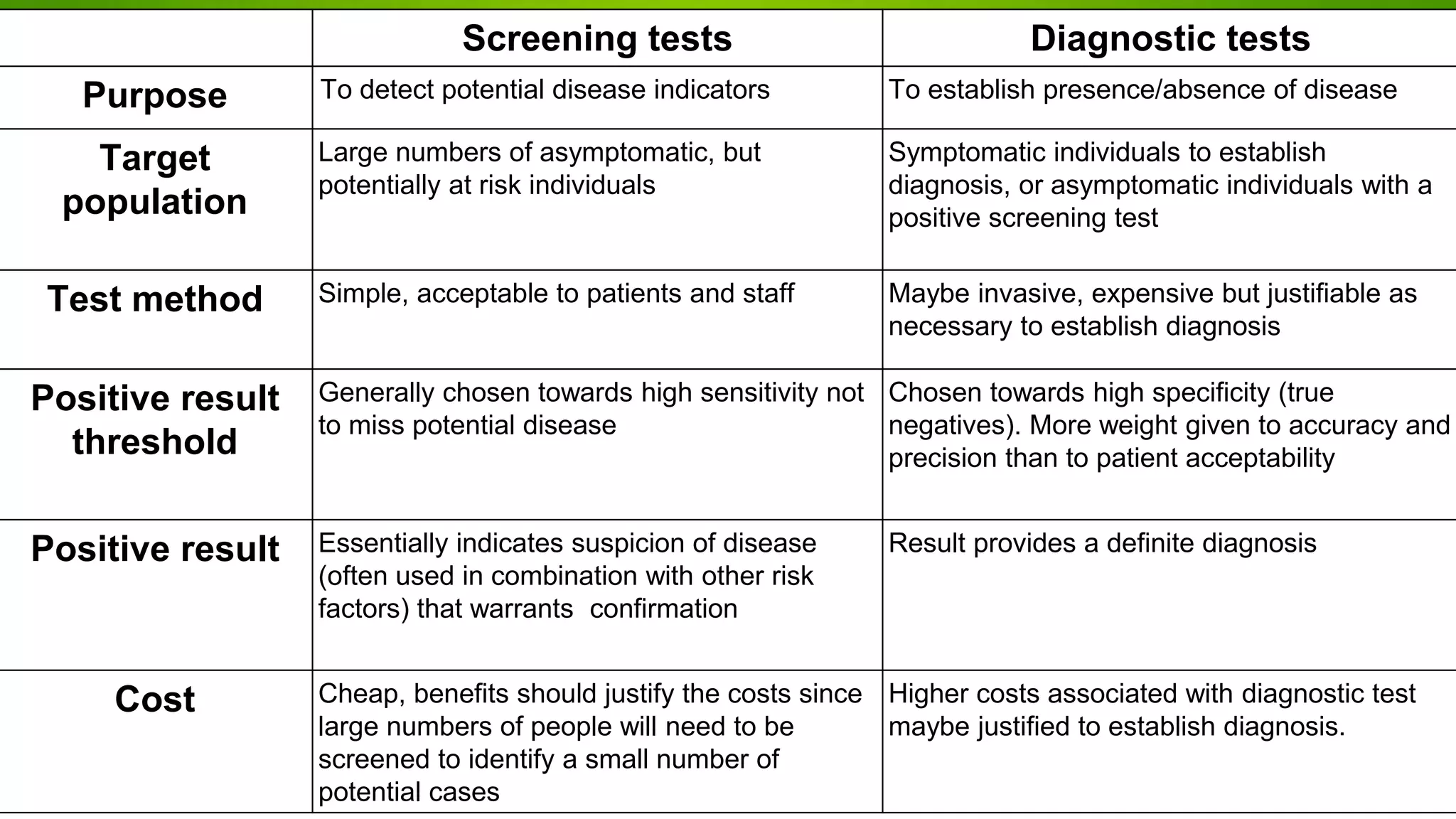
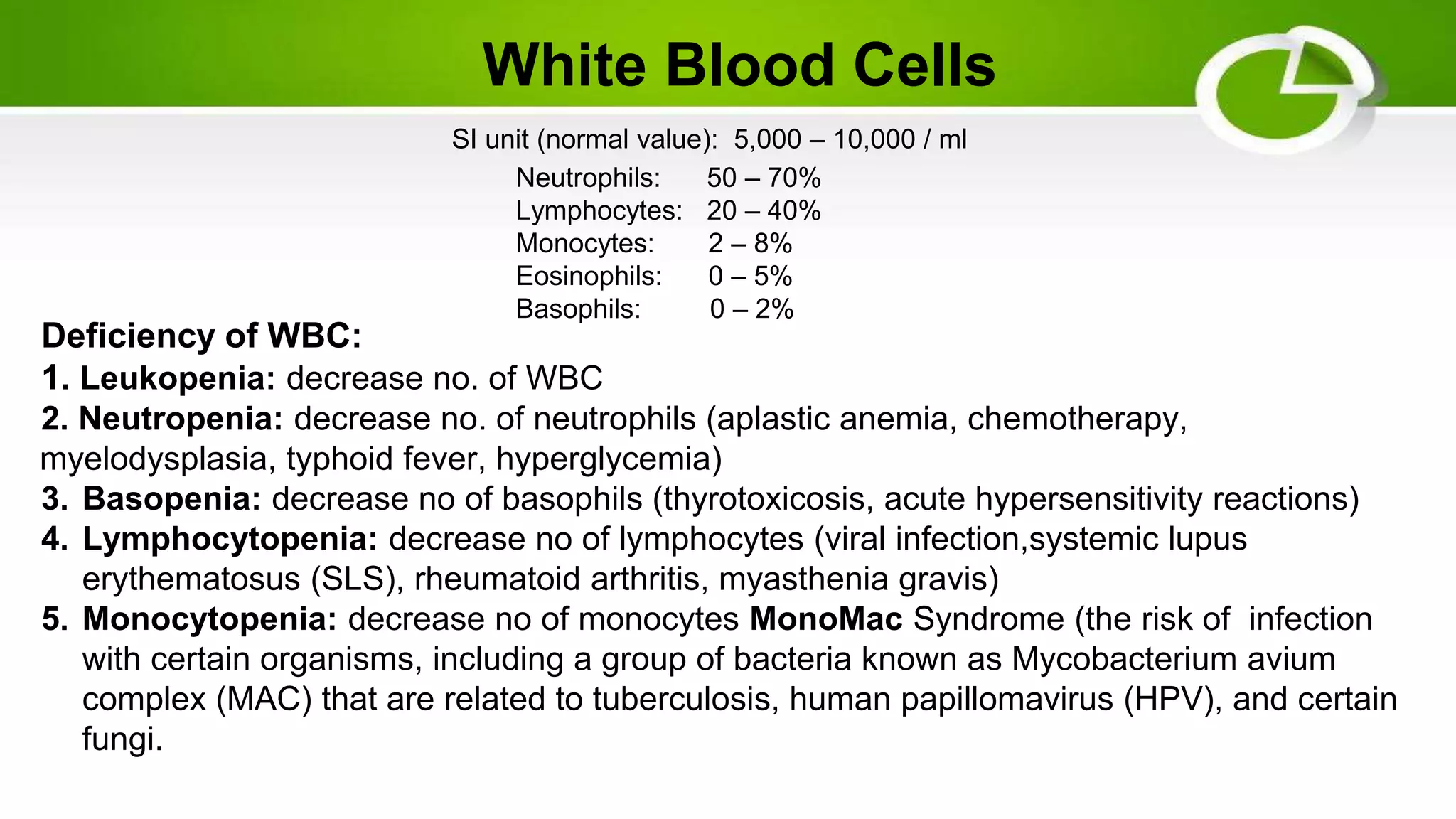
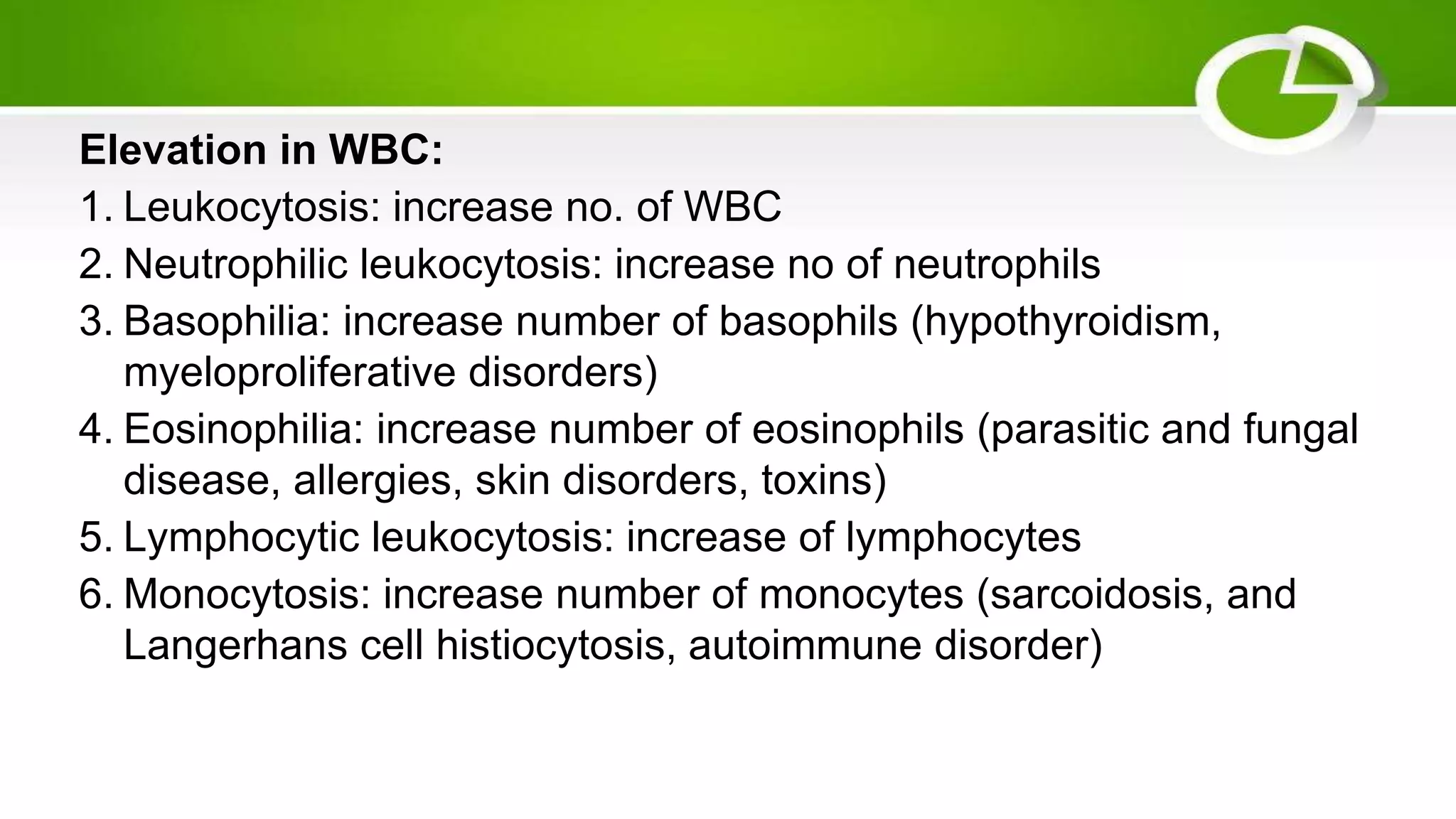
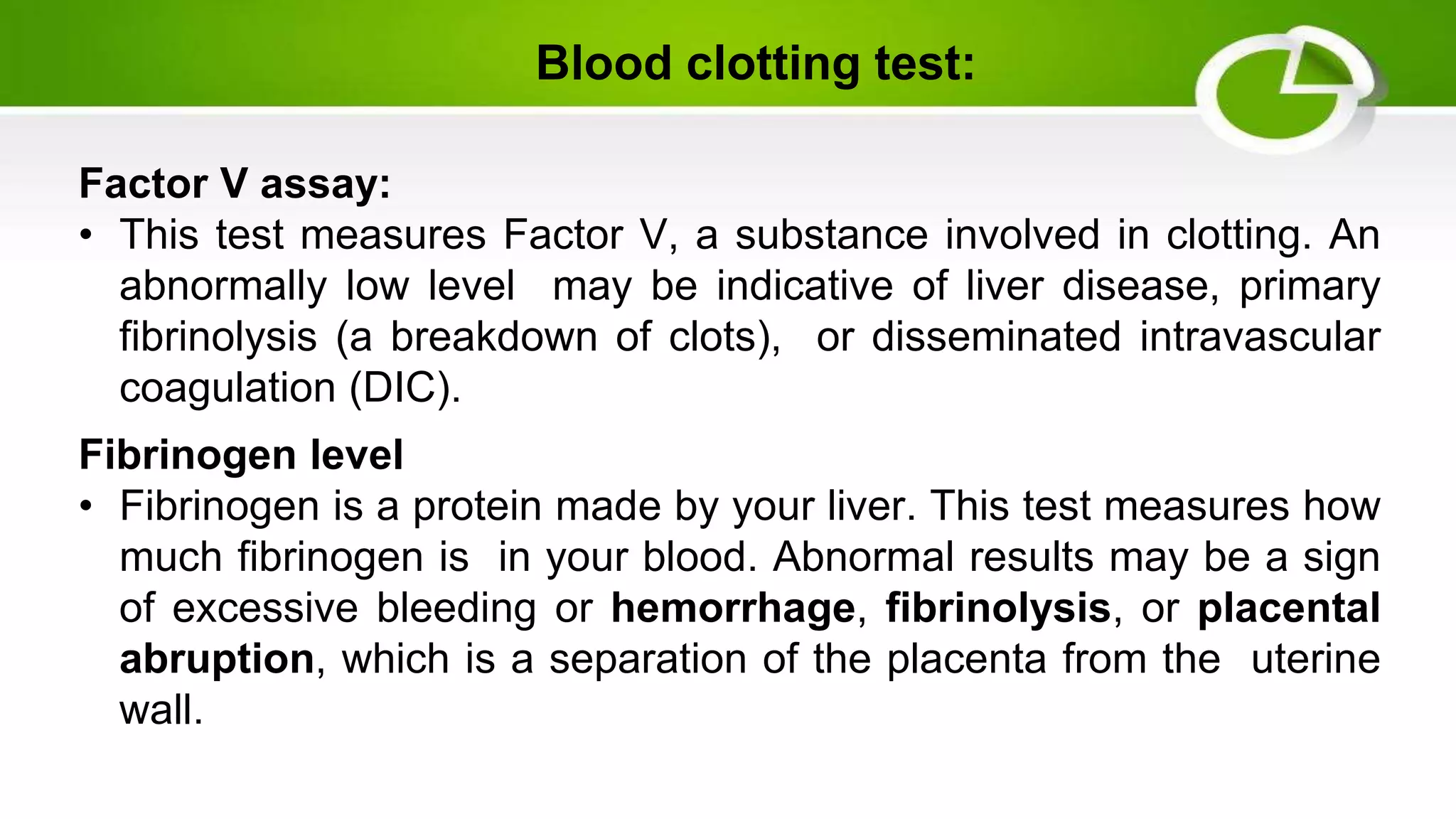
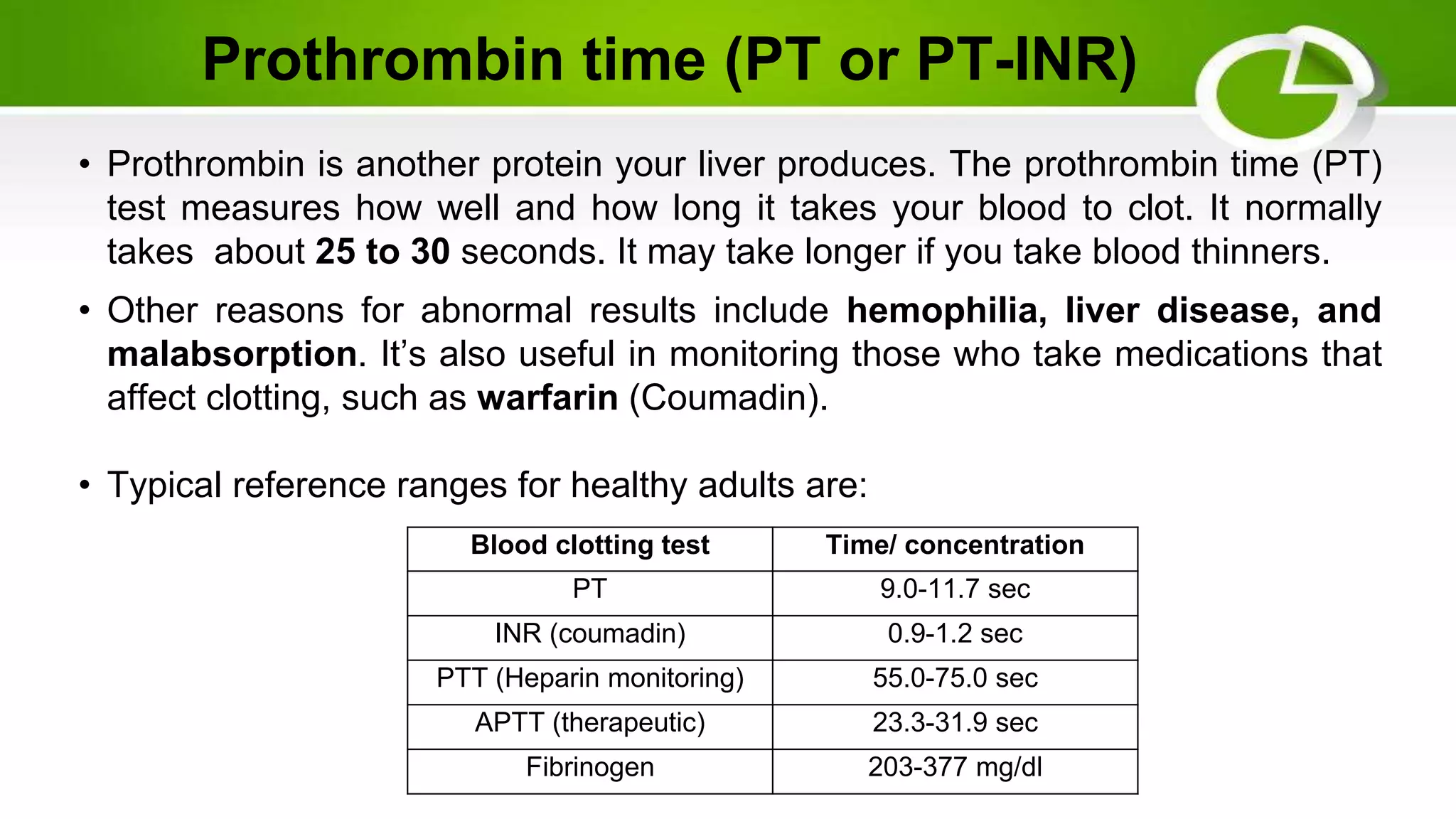
Laboratory tests help identify the nature of disease by examining tissues, blood, urine or other specimens. There are two main types of tests - screening tests which detect early disease in large populations, and diagnostic tests which confirm or rule out disease in symptomatic individuals. Hematology involves tests on blood and blood-forming organs to evaluate conditions like anemia, infection, blood cancers, and clotting disorders. Common hematology tests include complete blood count, coagulation profile, and tests that measure components of blood like red and white blood cells, hemoglobin, hematocrit, and platelets. Abnormal results can indicate various blood disorders and diseases.