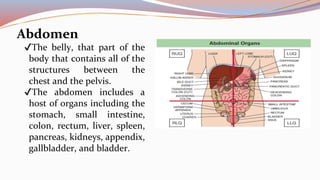
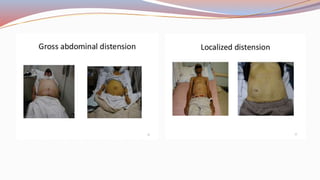
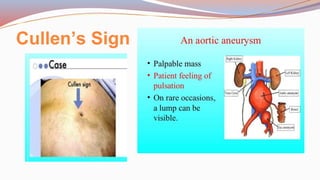
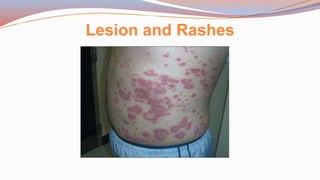
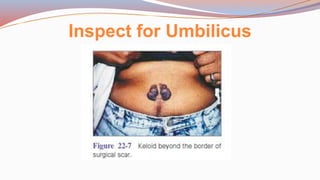
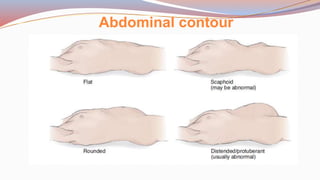
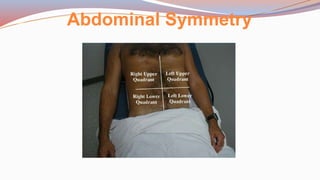
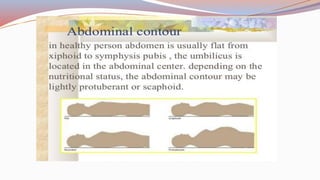
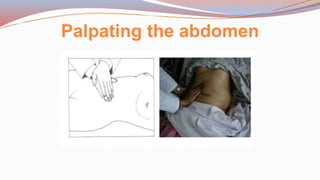
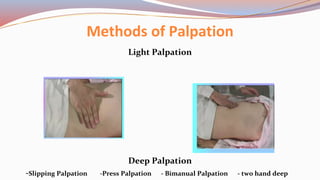
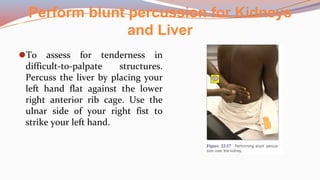
This document provides guidance on performing a physical assessment of the abdomen. It defines the abdomen and discusses the key steps in the abdominal exam, including inspection, auscultation, percussion, and palpation. Inspection involves visually examining the abdomen for things like shape, contour, symmetry, scars, and hernias. Auscultation listens for bowel sounds while percussion delineates organ borders by tapping. Palpation then feels the abdomen with light and deep pressure to check for tenderness, masses, pulsations, and organ size and consistency. The goal of the full abdominal exam is to thoroughly evaluate the abdominal structures and identify any abnormalities.