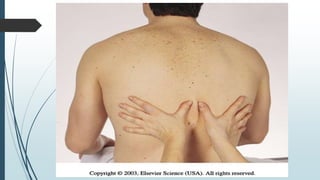
The document provides detailed information about the anatomy and landmarks of the chest, including the thoracic cage, ribs, sternum, and vertebrae. It describes the internal structures such as the lungs, heart, blood vessels, and pleura. Key points include that the left lung has two lobes instead of three, and the distribution of the different lung lobes in the anterior and posterior chest. The document also covers respiratory mechanics, auscultation locations and notes, palpation techniques, and abnormal chest findings.