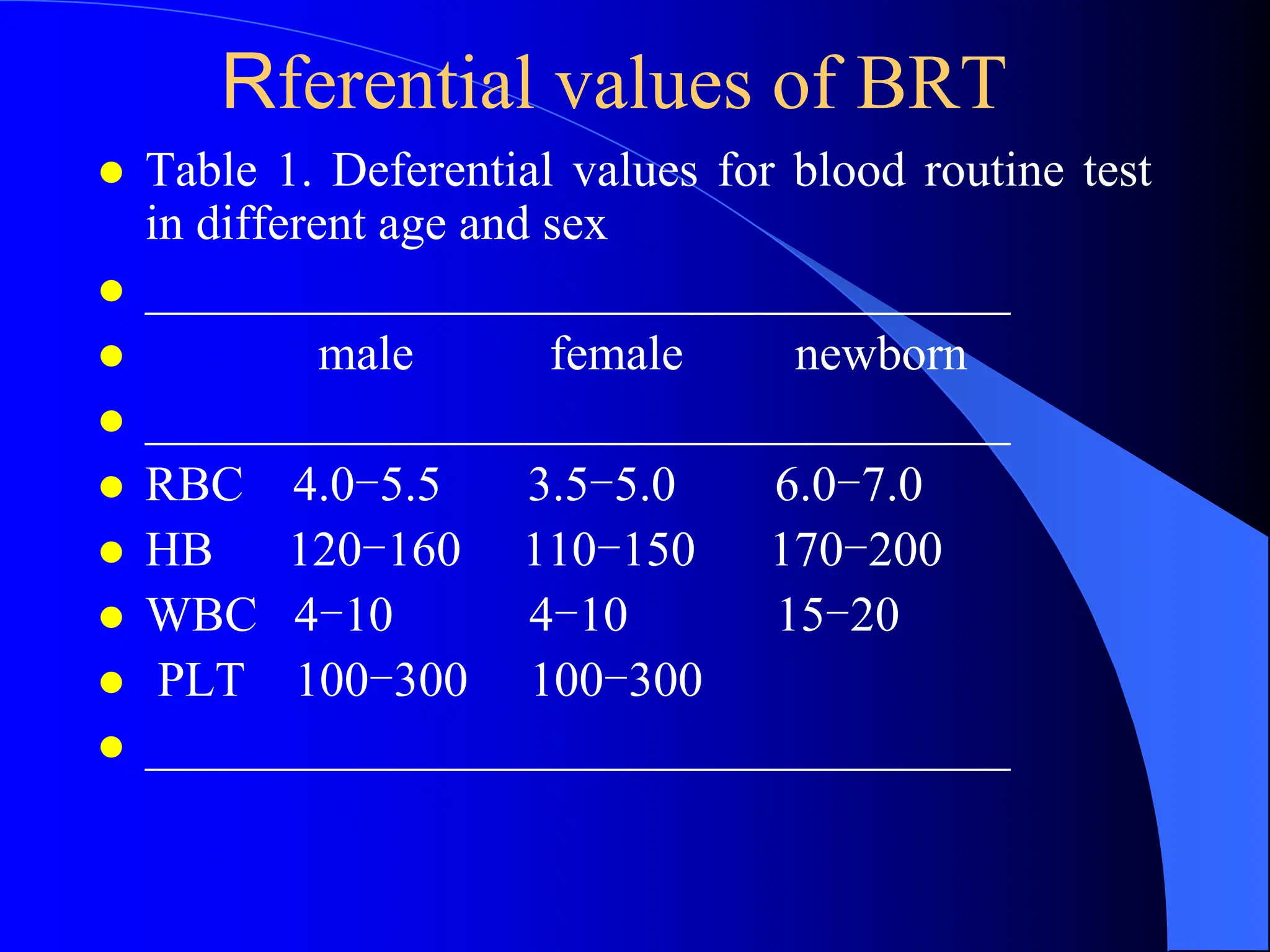
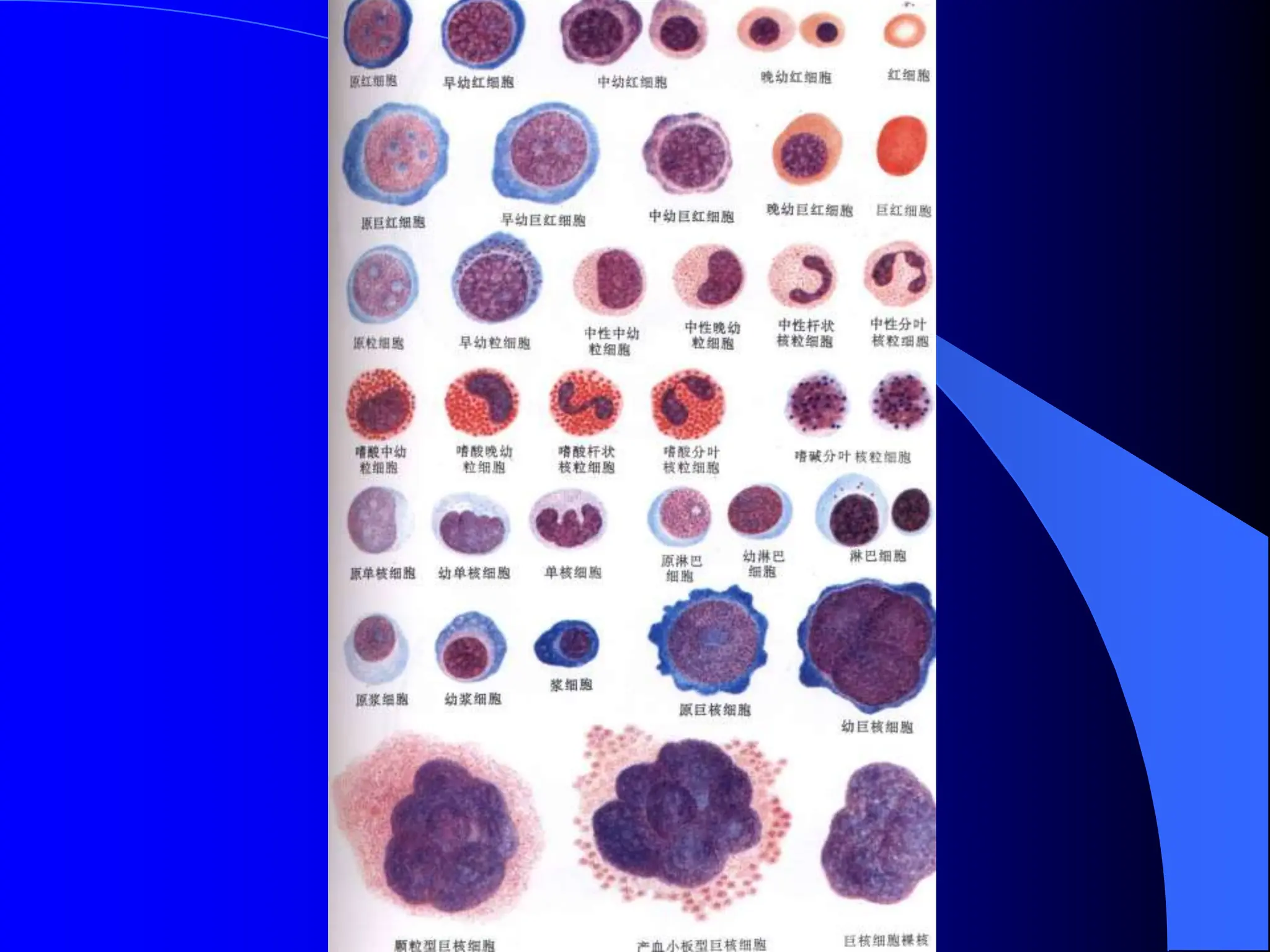
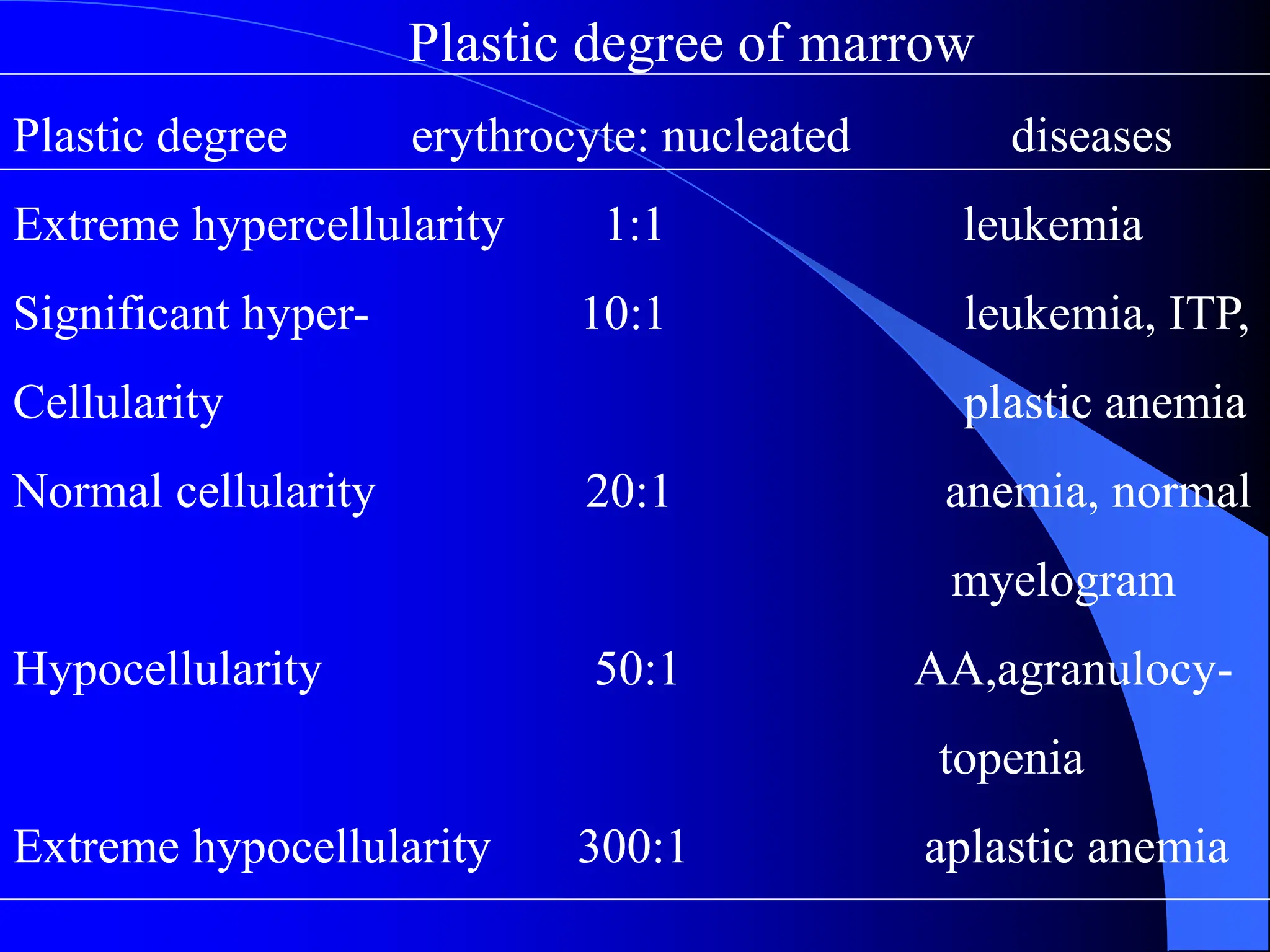
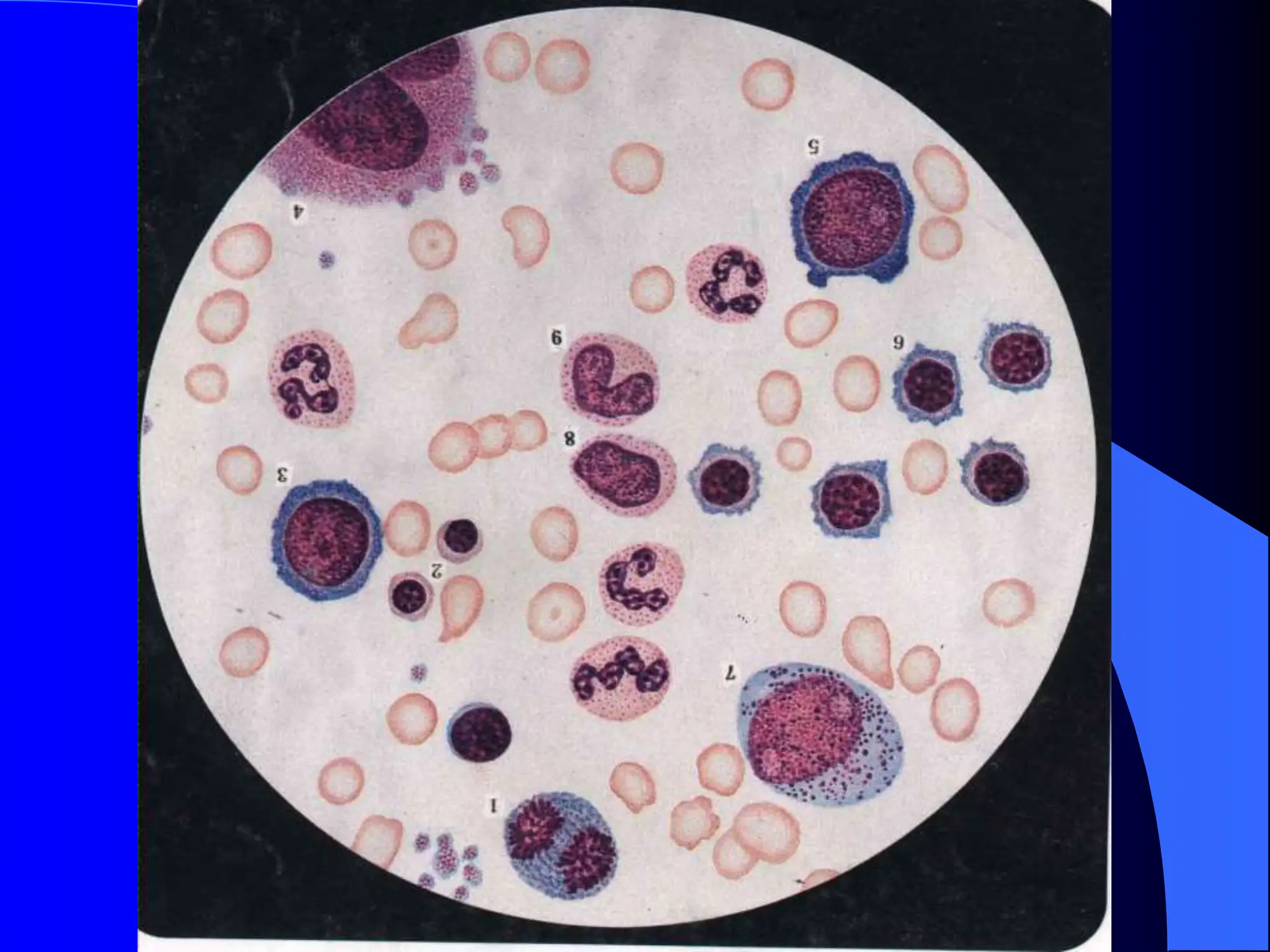
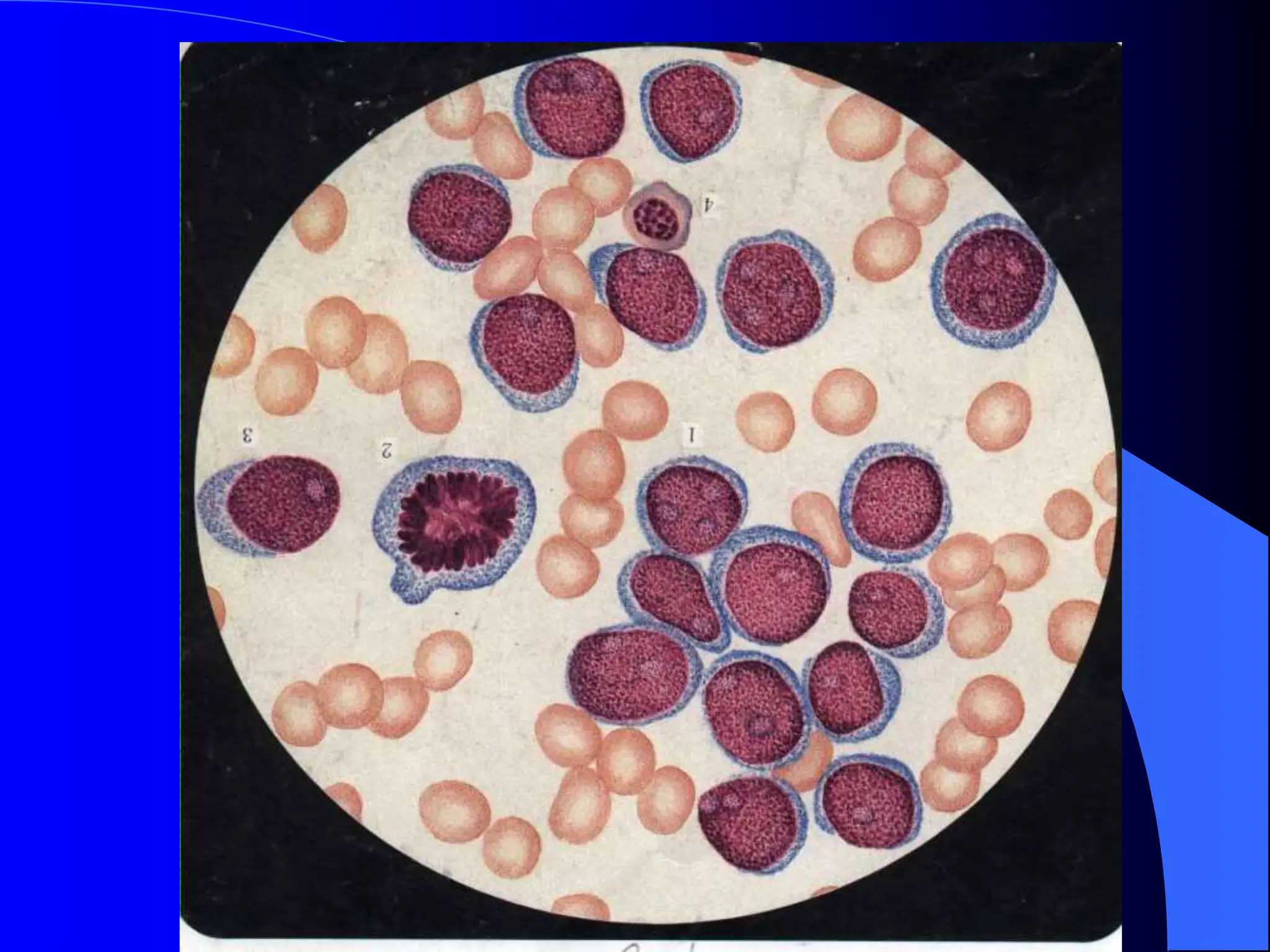
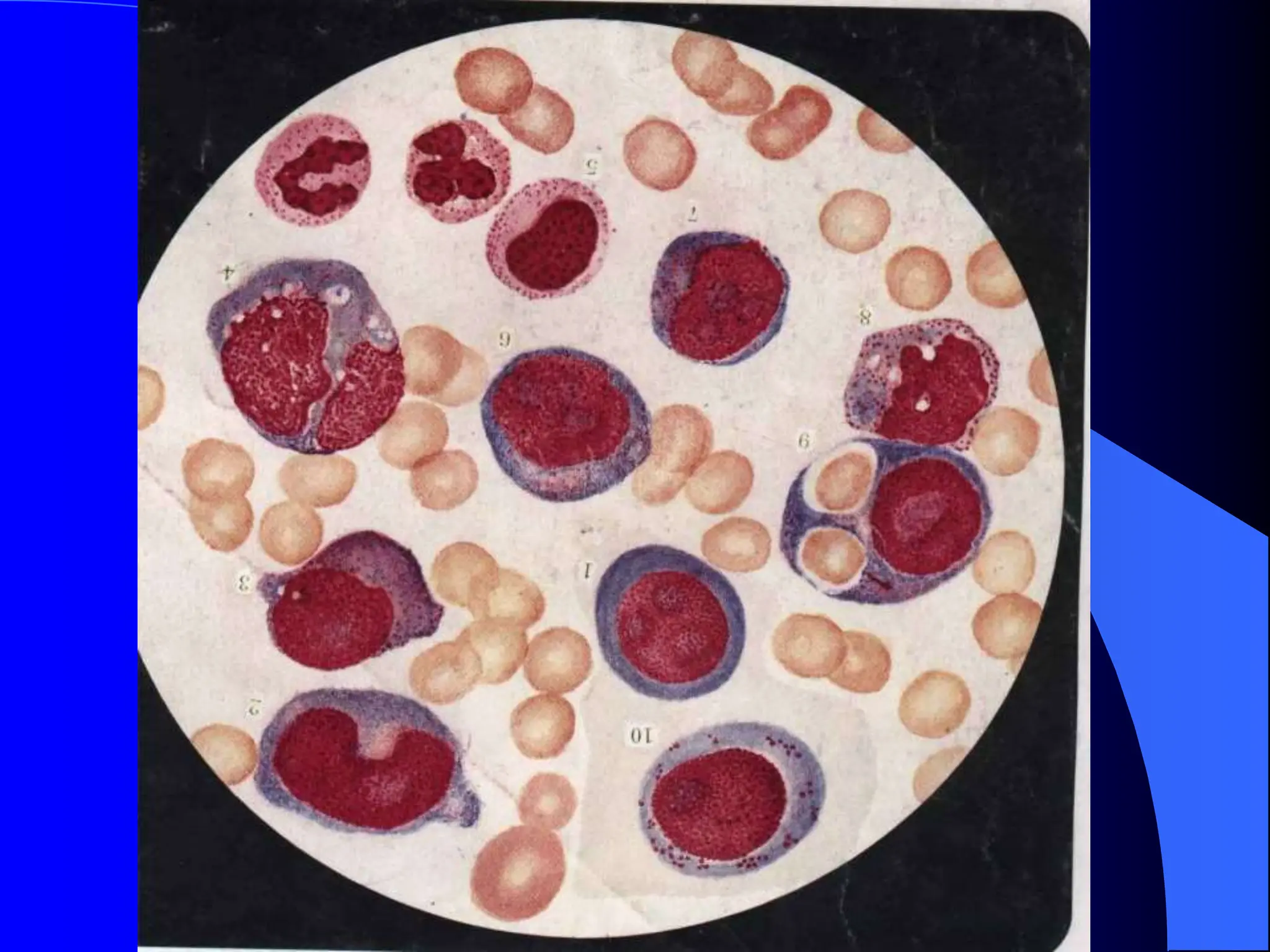
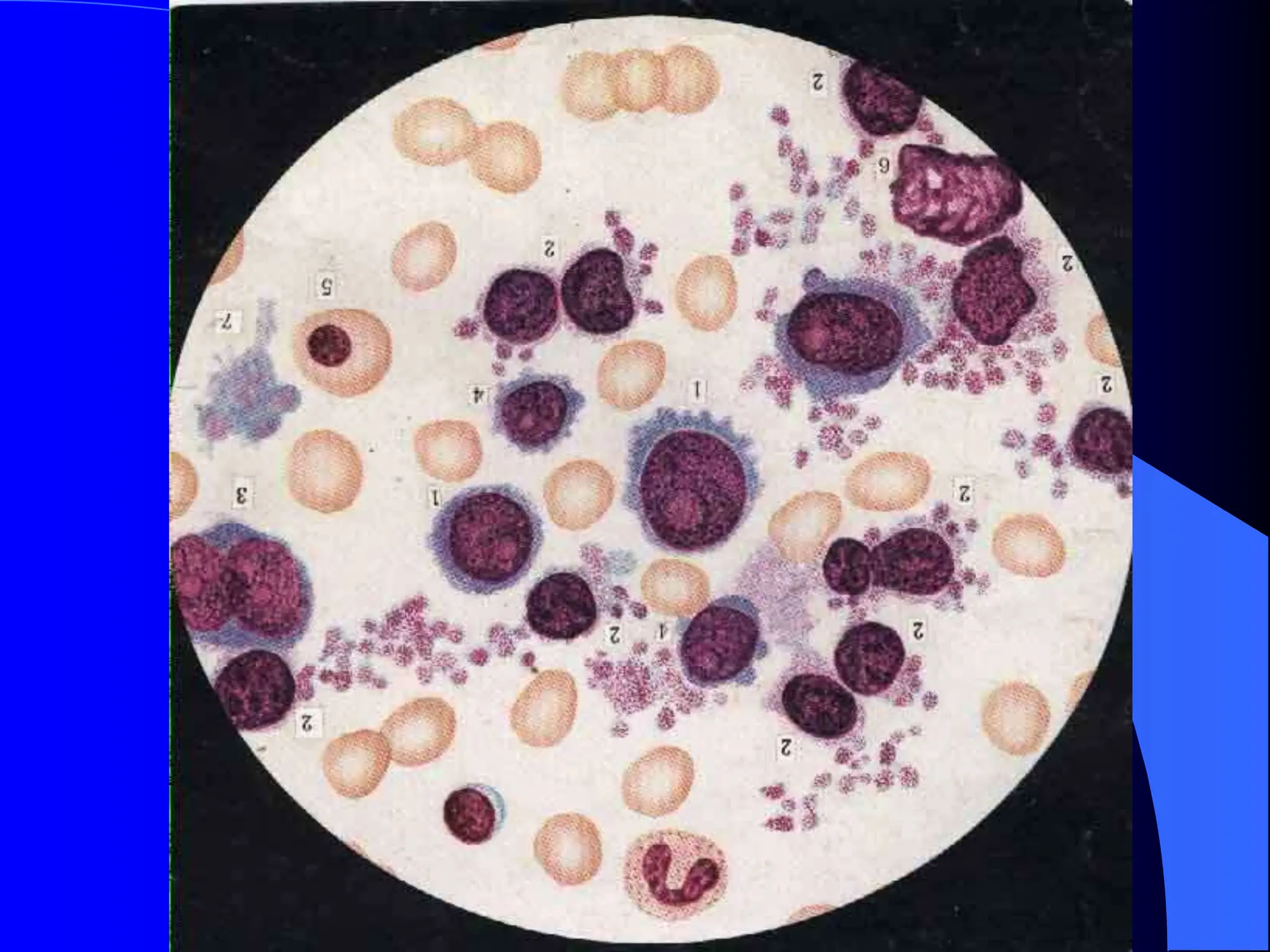
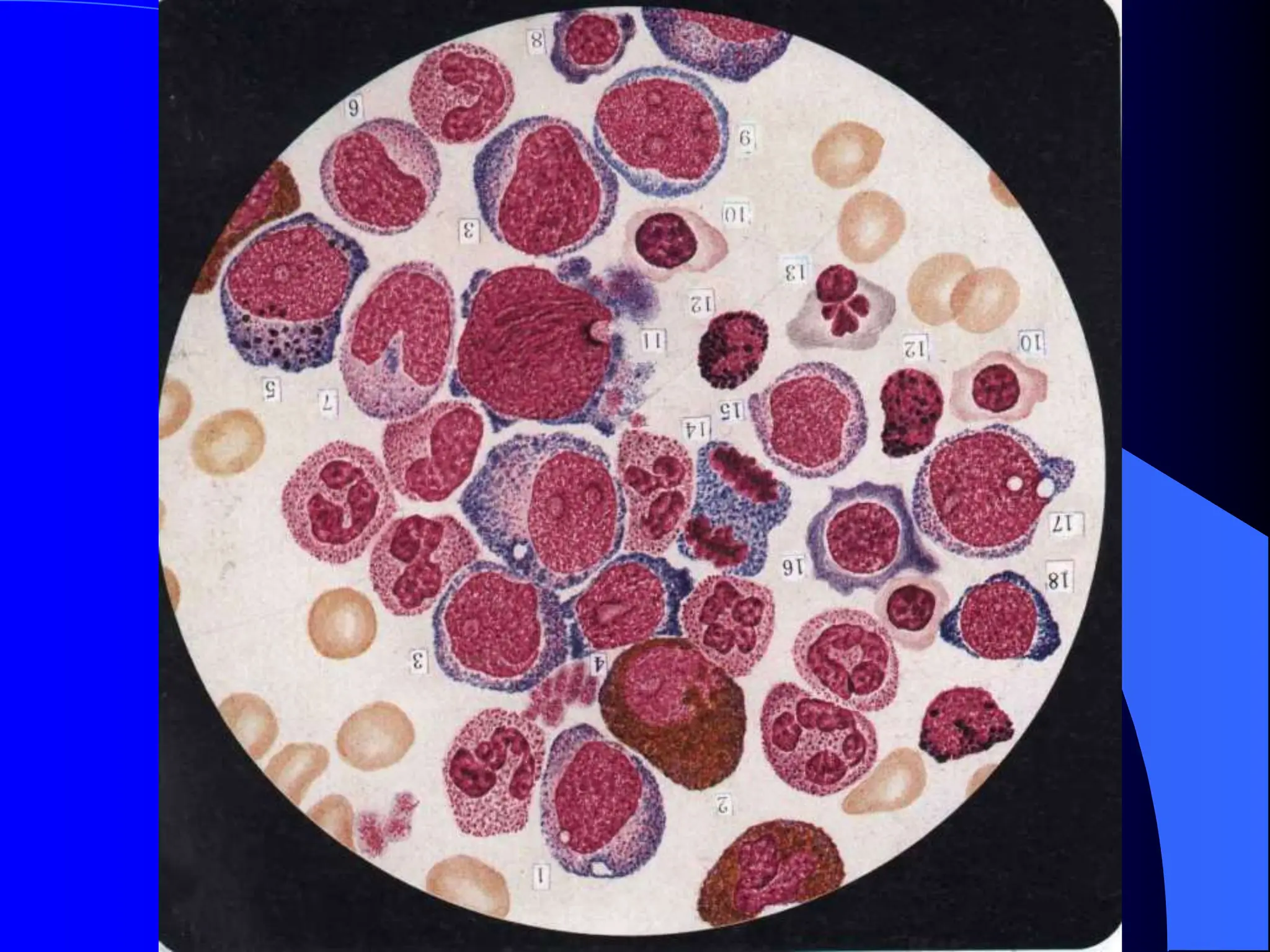
Laboratory diagnosis involves examining samples from patients to obtain diagnostic information. It is an important part of the diagnostic process that can help confirm or rule out potential diseases. Blood tests are a key part of laboratory diagnosis and can provide information on red blood cells, white blood cells, platelets, and other measures. Abnormal results may indicate conditions like anemia, infection, leukemia, or other blood disorders. Proper interpretation requires understanding reference values and clinical significance of each test result. Bone marrow examination can also help diagnose hematological conditions by examining cell development and morphology under a microscope.