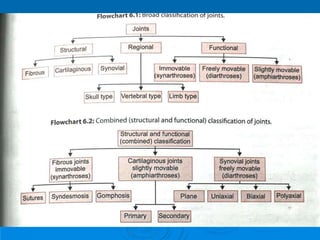
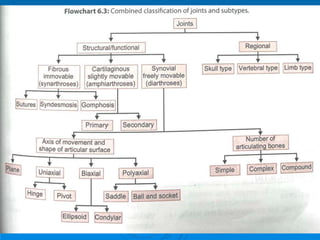
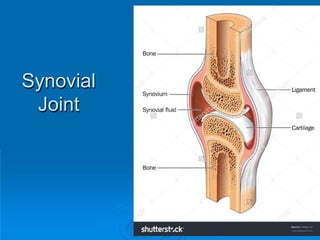
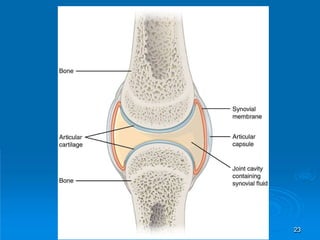
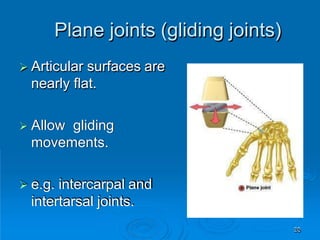
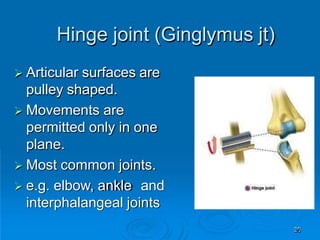
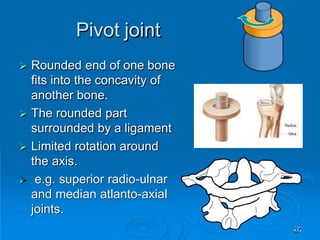
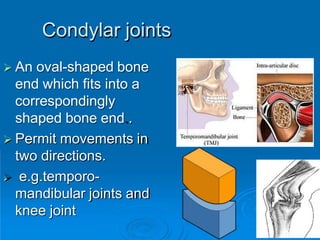
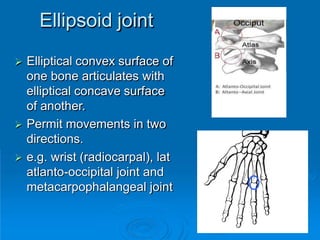
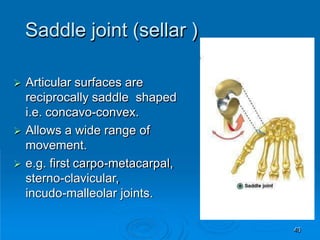
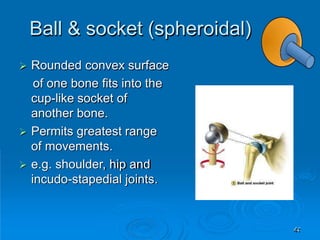
This document discusses the anatomy and classification of joints in the human body. It begins by defining joints and classifying them based on structure and movement. The main types of joints covered are fibrous, cartilaginous, and synovial joints. For synovial joints specifically, it describes the structures that make them up like the capsule, synovial membrane, articular cartilage, and ligaments. It then classifies synovial joints based on the shape of the articulating surfaces and degree of movement. Examples are provided throughout to illustrate the different joint types.