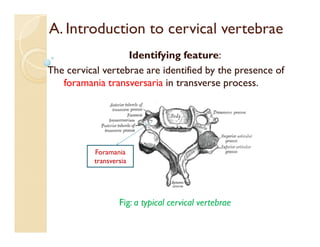
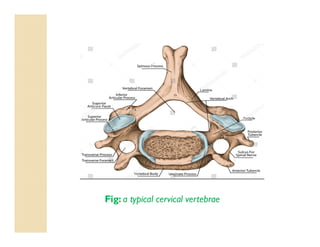
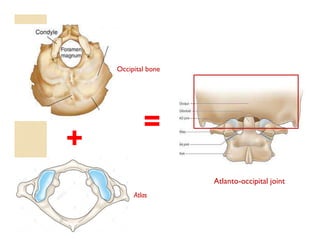
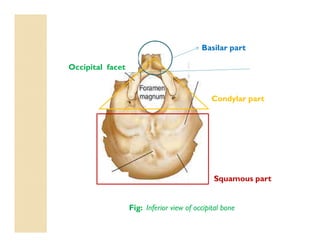
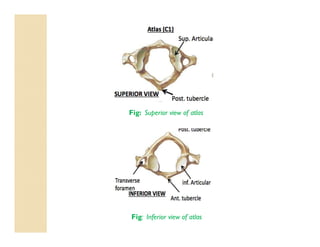
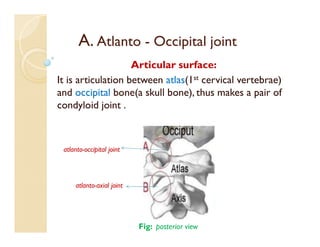
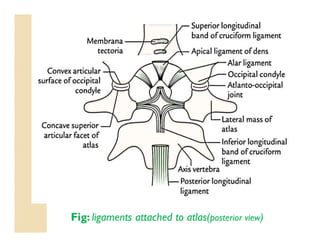
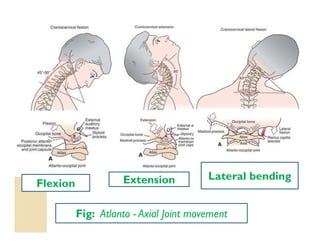
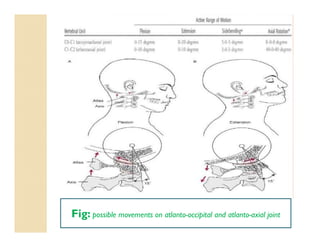
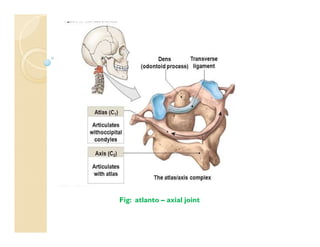
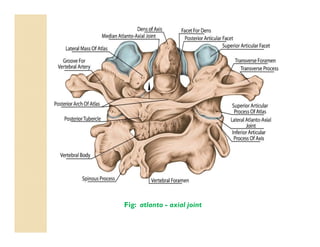
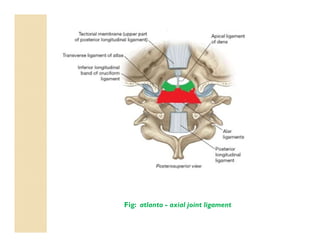
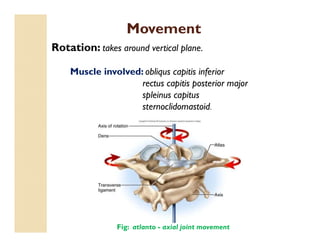
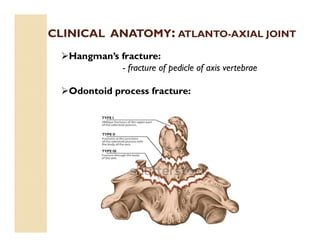
The document discusses the atlanto-occipital and atlanto-axial joints, including their anatomical characteristics, movements, and clinical implications. It covers the cervical vertebrae's features, the structure and function of the atlas and axis, and the types of movements possible at these joints. Additionally, it addresses conditions such as occipitalization of the atlas and various fractures associated with the atlanto-axial joint.