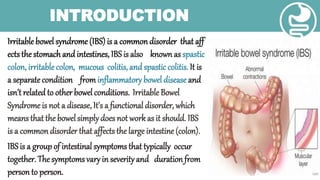
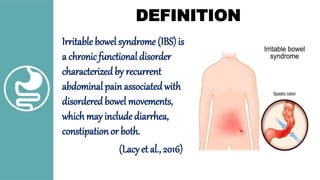
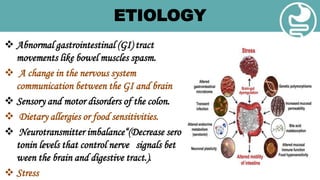
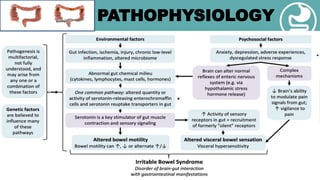

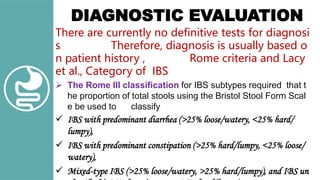
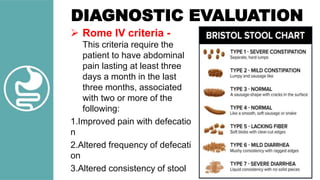


Irritable bowel syndrome (IBS) is a common functional disorder affecting the large intestine, characterized by recurrent abdominal pain and disordered bowel movements, prevalent in 3-22% of the population. Factors contributing to IBS include gastrointestinal tract irregularities, dietary sensitivities, mental health issues, and a familial tendency, with symptoms varying among individuals. Diagnosis is primarily based on patient history and symptoms, with management focusing on dietary changes, stress reduction techniques, and education on triggers.



































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















