Downloaded 49 times


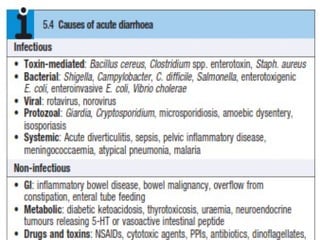

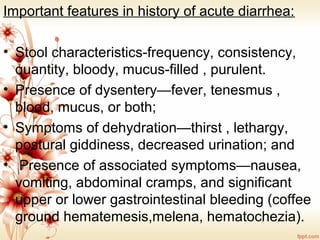

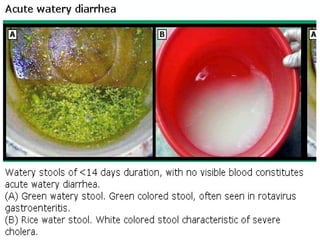

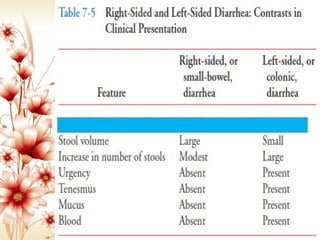



1) Acute diarrhea is usually infectious and self-limited, lasting less than 2 weeks. It can be classified as watery or bloody. Infectious causes include food poisoning, cholera, and shigellosis. 2) Chronic diarrhea lasts more than 4 weeks. It is often non-infectious, with irritable bowel syndrome being a common cause. Other potential organic causes include AIDS, diabetes, thyroid disease, or prior surgery. 3) Diarrhea is classified as acute vs chronic, small bowel vs colonic, and osmotic vs secretory based on characteristics like volume, response to fasting, and location of pathology.























































































