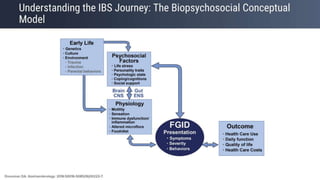
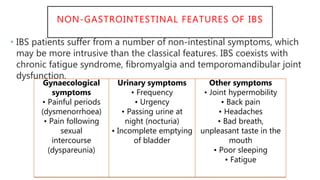
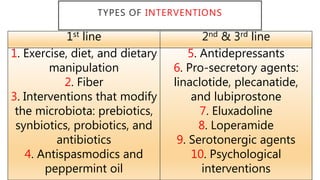
The document presents updates on the management of Irritable Bowel Syndrome (IBS), covering its definition, epidemiology, pathophysiology, diagnosis, and treatment interventions including lifestyle changes, medications, and psychological therapies. It highlights the importance of a biopsychosocial approach in managing IBS symptoms and emphasizes dietary modifications, particularly the low FODMAP diet, as an effective intervention. Guidelines from various health organizations are reviewed to provide evidence-based recommendations on IBS management.
![GUIDELINES REVIEWED
• World Gastroenterology Organisation Global Guidelines - Irritable
Bowel Syndrome: a Global Perspective [WGO]
• American College of Gastroenterologists Clinical Guideline:
Management of Irritable Bowel Syndrome [ACG]
• British Society of Gastroenterology guidelines on the management of
irritable bowel syndrome [BSG]
• NICE Irritable bowel syndrome in adults: diagnosis and management
• Canadian Association of Gastroenterology Clinical Practice Guideline
for the Management of Irritable Bowel Syndrome](https://image.slidesharecdn.com/ibsmanagementupdate-220301145240/85/IBS-Irritable-Bowel-Syndrome-Management-Update-2021-3-320.jpg)
![NICE ABC MNEMONIC FOR DIAGNOSIS
• The diagnosis of IBS should be considered if the patient has had the
following for at least 6 months:
• Abdominal pain, and/or
• Bloating, and/or
• Change in bowel habit
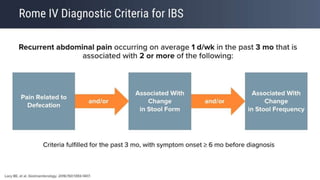
“Although the Rome IV criteria are the gold standard to define IBS for research purposes,
they are probably overly restrictive for use, even in secondary care, and a pragmatic
definition in line with that used in the NICE guideline, and outlined above, should be
preferred.” [BSG]](https://image.slidesharecdn.com/ibsmanagementupdate-220301145240/85/IBS-Irritable-Bowel-Syndrome-Management-Update-2021-14-320.jpg)

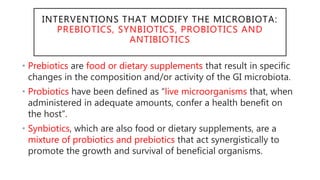
![INTERVENTIONS THAT MODIFY THE MICROBIOTA:
PREBIOTICS, SYNBIOTICS, PROBIOTICS AND
ANTIBIOTICS
• Guidelines suggest against the use of prebiotics and synbiotics for
overall symptom improvement in IBS patients.
• All Guidelines suggest probiotics, taken as a group, to improve
global symptoms, as well as bloating and flatulence in IBS patients.
• It is reasonable to advise patients wishing to try probiotics to take
them for up to 12 weeks, and to discontinue them if there is no
improvement in symptoms. [BSG]
• ACG suggest the non-absorbable antibiotic rifaximin for reduction in
global IBS symptoms, as well as bloating in non-constipated IBS
patients.](https://image.slidesharecdn.com/ibsmanagementupdate-220301145240/85/IBS-Irritable-Bowel-Syndrome-Management-Update-2021-31-320.jpg)
![DRUGS USED FIRST LINE FOR IBS -
ANTISPASMODICS AND PEPPERMINT OIL
• All guidelines suggest Certain antispasmodics [antimuscarinics
and smooth muscle relaxants- (trimebutine- TRITIN, otilonium, hyoscine,
cimetropium, pinaverium, dicyclomine and mebeverine, alverine citrate- ALRIN]
as an effective treatment for global symptoms and
abdominal pain in IBS. Dry mouth, visual disturbance and
dizziness are common side effects.
• All guidelines suggest Peppermint oil as an effective
treatment for global symptoms and abdominal pain in IBS.
Gastro-oesophageal reflux is a common side effect. The risk
of adverse events is no greater with peppermint oil than
with a placebo.](https://image.slidesharecdn.com/ibsmanagementupdate-220301145240/85/IBS-Irritable-Bowel-Syndrome-Management-Update-2021-32-320.jpg)
![GUT BRAIN MODULATORS
TCA AND SSRI
• TCAs and SSRIs impact on bowel function, with TCAs improving diarrhea
by slowing GI transit, and SSRIs ameliorating constipation by accelerating
GI transit.
• Tricyclic antidepressants used as gut-brain neuromodulators are an
effective second-line drug for global symptoms and abdominal pain in
IBS. [BSG]
• They should be commenced at a low dose (eg, 10 mg amitriptyline once a
day) and titrated slowly to a maximum of 30–50 mg once a day. [BSG]
• TCAs are associated with significant adverse effects in treating IBS-D and
should be avoided in IBS-C; clinicians should expect one adverse effect for
every three patients who benefit from therapy [WGO]](https://image.slidesharecdn.com/ibsmanagementupdate-220301145240/85/IBS-Irritable-Bowel-Syndrome-Management-Update-2021-35-320.jpg)
![GUT BRAIN MODULATORS
TCA AND SSRI
• SSRIs may be considered in resistant IBS-C, although it is not
currently recommended that SSRIs should be routinely prescribed for
IBS in patients without comorbid psychiatric conditions. [WGO]
• Selective serotonin reuptake inhibitors used as gut-brain
neuromodulators may be an effective second-line drug for global
symptoms in IBS. [BSG/ ACG]
• Whether all IBS sufferers, or only certain sub-populations, respond to
anti-depressants is also unclear, and therapy with these agents may
be limited by patient acceptance and adverse events.](https://image.slidesharecdn.com/ibsmanagementupdate-220301145240/85/IBS-Irritable-Bowel-Syndrome-Management-Update-2021-36-320.jpg)
![DRUGS USED SECOND LINE FOR THE
TREATMENT OF IBS-D
• Who do not experience symptom improvement with antidiarrhoeals
• 5-Hydroxytryptamine 3 receptor antagonists are efficacious second-
line drugs for IBS with diarrhoea in secondary care. [Ondansetron
titrated from a dose of 4 mg once a day to a maximum of 8 mg tds]
Constipation is the most common side effect. (EMEREN/EMESET)
• The non-absorbable antibiotic rifaximin is an efficacious second-line
drug for IBS with diarrhoea in secondary care.
• Other options- Eluxadoline, a mixed opioid receptor drug;
contraindicated in patients with cholecystectomy, pancreatitis or
severe liver impairment](https://image.slidesharecdn.com/ibsmanagementupdate-220301145240/85/IBS-Irritable-Bowel-Syndrome-Management-Update-2021-37-320.jpg)
![PSYCHOLOGICAL THERAPIES
• All guidelines suggest IBS-specific cognitive behavioural therapy as an
efficacious treatment for global symptoms in IBS.
• Psychological therapies should be considered when symptoms have not
improved after 12 months of drug treatment. [BSG]
• General nonpharmacological recommendations
• Discuss the patient’s anxieties. This reduces complaints; aim to eliminate
unnecessary worries.
• Aim to reduce avoidance behavior. Patients may avoid activities that they fear
are causing the symptoms, but avoidance behavior has a negative influence on
the prognosis.
• Discuss and aim to resolve stressful factors.](https://image.slidesharecdn.com/ibsmanagementupdate-220301145240/85/IBS-Irritable-Bowel-Syndrome-Management-Update-2021-39-320.jpg)