




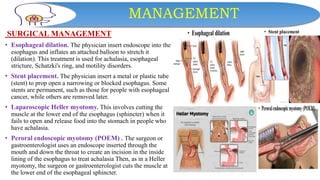
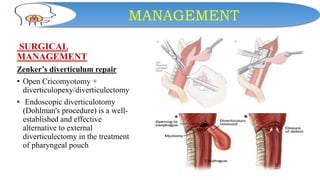


This document discusses dysphagia, or difficulty swallowing. It begins by defining dysphagia and describing the normal physiology of swallowing in three stages. It then discusses the various types, causes, signs and symptoms, diagnostic tests, complications and management approaches for dysphagia. Management may include dietary changes, swallowing exercises and techniques, botulinum toxin injections, dilation procedures, or surgeries like myotomy. Nurses play an important role in educating patients and monitoring for signs of aspiration during meals.























































































