Intestinal Flagellates notes 2014
•
10 likes•2,710 views

This document summarizes several intestinal and urogenital flagellates including Giardia lamblia, Trichomonas vaginalis, Dientamoeba fragilis, Trichomonas tenax, Chilomastix mesnili, Retortamonas intestinalis, and Trichomonas hominis. It describes the morphology, life cycles, transmission routes, clinical manifestations, diagnosis, treatment and prevention of these parasites. Giardia lamblia is a common cause of parasitic diarrhea and is transmitted through ingestion of cysts from contaminated food, water or surfaces. Trichomonas vaginalis causes the sexually transmitted infection trichomoniasis through sexual contact.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (13)
Similar to Intestinal Flagellates notes 2014
Similar to Intestinal Flagellates notes 2014 (20)
More from Medina College
More from Medina College (18)
Recently uploaded
Recently uploaded (20)
Intestinal Flagellates notes 2014
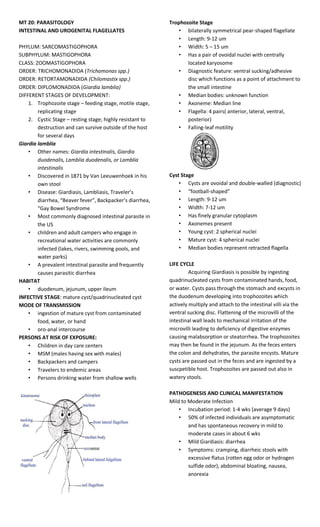
- 1. MT 20: PARASITOLOGY INTESTINAL AND UROGENITAL FLAGELLATES PHYLUM: SARCOMASTIGOPHORA SUBPHYLUM: MASTIGOPHORA CLASS: ZOOMASTIGOPHORA ORDER: TRICHOMONADIDA (Trichomonas spp.) ORDER: RETORTAMONADIDA (Chilomastix spp.) ORDER: DIPLOMONADIDA (Giardia lamblia) DIFFERENT STAGES OF DEVELOPMENT: 1. Trophozoite stage – feeding stage, motile stage, replicating stage 2. Cystic Stage – resting stage; highly resistant to destruction and can survive outside of the host for several days Giardia lamblia • Other names: Giardia intestinalis, Giardia duodenalis, Lamblia duodenalis, or Lamblia intestinalis • Discovered in 1871 by Van Leeuwenhoek in his own stool • Disease: Giardiasis, Lambliasis, Traveler’s diarrhea, “Beaver fever”, Backpacker’s diarrhea, “Gay Bowel Syndrome • Most commonly diagnosed intestinal parasite in the US • children and adult campers who engage in recreational water activities are commonly infected (lakes, rivers, swimming pools, and water parks) • A prevalent intestinal parasite and frequently causes parasitic diarrhea HABITAT • duodenum, jejunum, upper ileum INFECTIVE STAGE: mature cyst/quadrinucleated cyst MODE OF TRANSMISSION • ingestion of mature cyst from contaminated food, water, or hand • oro-anal intercourse PERSONS AT RISK OF EXPOSURE: • Children in day care centers • MSM (males having sex with males) • Backpackers and campers • Travelers to endemic areas • Persons drinking water from shallow wells Trophozoite Stage • bilaterally symmetrical pear-shaped flagellate • Length: 9-12 um • Width: 5 – 15 um • Has a pair of ovoidal nuclei with centrally located karyosome • Diagnostic feature: ventral sucking/adhesive disc which functions as a point of attachment to the small intestine • Median bodies: unknown function • Axoneme: Median line • Flagella: 4 pairs( anterior, lateral, ventral, posterior) • Falling-leaf motility Cyst Stage • Cysts are ovoidal and double-walled (diagnostic) • “football-shaped” • Length: 9-12 um • Width: 7-12 um • Has finely granular cytoplasm • Axonemes present • Young cyst: 2 spherical nuclei • Mature cyst: 4 spherical nuclei • Median bodies represent retracted flagella LIFE CYCLE Acquiring Giardiasis is possible by ingesting quadrinucleated cysts from contaminated hands, food, or water. Cysts pass through the stomach and excysts in the duodenum developing into trophozoites which actively multiply and attach to the intestinal villi via the ventral sucking disc. Flattening of the microvilli of the intestinal wall leads to mechanical irritation of the microvilli leading to deficiency of digestive enzymes causing malabsorption or steatorrhea. The trophozoites may then be found in the jejunum. As the feces enters the colon and dehydrates, the parasite encysts. Mature cysts are passed out in the feces and are ingested by a suscpetible host. Trophozoites are passed out also in watery stools. PATHOGENESIS AND CLINICAL MANIFESTATION Mild to Moderate Infection • Incubation period: 1-4 wks (average 9 days) • 50% of infected individuals are asymptomatic and has spontaneous recovery in mild to moderate cases in about 6 wks • Mild Giardiasis: diarrhea • Symptoms: cramping, diarrheic stools with excessive flatus (rotten egg odor or hydrogen sulfide odor), abdominal bloating, nausea, anorexia
- 2. Severe to Chronic Infection • Severe cases causes malabsorption and steatorrhea • Flattening of the tips of the microvilli and shallow crypts • With inflammation of the mucosa and hyperplasia of lymphoid follicles • Ventral sucking disc causes flattening of the microvilli leading to deficiency of digestive enzymes causing steatorrhea and malabsorption • Passage of greasy, frothy stools that float on toilet water • Weight loss, generalized weakness, chills, and low grade fever LABORATORY DIAGNOSIS • Demonstration of trophozoite and cyst in stools specimens via direct fecal smear – 3 Stool exams on alternate days to increase sensitivity • Duodenal aspirate or biopsy – if parasite is not found in the feces; demonstrates trophozoites • Entero-test/Entero-string test: demonstrates Giardia lamblia trophozoites – Higher sensitivity; accurate, and inexpensive – Specimen: duodenal fluid – Makes use of a gelatin capsule Serologic Tests: • Direct Fluorescent Antibody • ELISA – to detect Giardia-specific antigen – High sensitivity TREATMENT • Metronidazole • Tinidazole • Furazolidone EPIDEMIOLOGY • Associated with poor environmental sanitation • Giardia is found worldwide and infects domestic and wild animals (e.g., cats, dogs, cattle, deer, and beavers) • Waterborne outbreaks are associated with ingestion of both drinking and recreational water • Foodborne outbreaks have also been reported RISK FACTORS • Poor hygiene and sanitation • Overcrowding (mental institutions, day care centers) • Immunodeficiency • Bacterial and fungal overgrowth in the small intestine • Homosexual practices PREVENTION AND CONTROL • Proper and sanitary disposal of human excreta • Stop using night soil as fertilizer – resp. for contaminated food Dientamoeba fragilis D. fragilis is believed to be transmitted between human hosts inside helminth eggs or larvae, particularly those of Enterobius vermicularis and Ascaris lumbricoides. DNA of D. fragilis is found in these helminth ova. It frequently infects children. The complete life cycle of this parasite has not yet been determined, but assumptions were made based on clinical data. To date, the cyst stage has not been identified in D. fragilis life cycle, and the trophozoite is the only stage found in stools of infected individuals. D. fragilis is probably transmitted by fecal-oral route and transmission via helminth eggs (e.g., Ascaris, Enterobius spp.) has been postulated. Trophozoites of D. fragilis have characteristically one or two nuclei, and it is found in children complaining of intestinal (e.g., intermittent diarrhea, abdominal pain) and other symptoms (e.g., nausea, anorexia, fatigue, malaise, poor weight gain). CLINICAL MANIFESTATIONS diarrhea, abdominal pain, anorexia, nausea, vomiting, fatigue, and weight loss. LABORATORY DIAGNOSIS Detection of trophozoites in permanently stained fecal smears (e.g., trichrome) This parasite is not detectable by stool concentration methods. TREATMENT Iodoquinol – DOC Paromomycin Tetracycline (contraindicated in children under age 8, pregnant and lactating women) Metronidazole _______________________________________ Trichomonas vaginalis • Disease: Trichomoniasis (STD) • Common Name: Trich • The only pathogenic specie in the genus • Discovered by Donne in 1836 in purulent secretion of male urogenital discharge and female vaginal discharge • Exists only in the trophozoite stage
- 3. Trophozoite • Pyriform shape; tear-drop shape** • Length: 7-23 um • 4 anterior flagella • 5th flagellum is embedded in the undulating membrane or axostyle; has barbwire-like appearance and is responsible for attachment and tearing up of the vaginal wall which causes inflammation and intensifying the infection • Undulating membrane** extends halfway through the body of the parasite; this structure is resp. for sweeping nutrients into the cytostome • Has a single nucleus that’s anteriorly located • Has an axostyle that extends throughout the length of the body and projects posteriorly • Has chromatin/siderophil granules in the cytoplasm but more prominent in the costa and axostyle • Lacks mitochondria but is replaced by hydrogenosome which produces ATP HABITAT • Males: urogenital tract (urethra, pelvis, prostate, epididymis) • Females: vagina ascending to the renal pelvis REPRODUCTION • Longitudinal Binary fission MODE OF TRANSMISSION • Sexual intercourse LIFE CYCLE • The trophozoites live in the urinary or reproductive tracts until they are passed onto their next human host via unprotected sexual contact, where the whole process starts over again. PATHOGENESIS AND CLINICAL MANIFESTATION FEMALES • Inflammation of the vaginal mucosa • T. vaginalis are not free living organisms • Requires human host • Women will show symptoms of being infected between five and 28 days after exposure. • Irritation, inflammation, burning, itching, and a smelly, frothy, discharge, ranging from green to yellow to gray are indications of a T. vaginalis infection. • Sores will sometimes be present as well, from the T. vaginalis' barbwire-like flagella. • Vulvitis and dysuria • Increased incidence of Trichomoniasis in postpartum endometritis • Strawberry cervix MALES • Asymptomatic and latent infection • Responsible for persistent/recurring urethritis • Most common complication: Prostatitis • Itching and discomfort inside the penile urethra esp. during urination LABORATORY DIAGNOSIS MALES • Demonstration of trophozoite in urine, urethral discharge, prostatic secretions in wet mounts FEMALES • Demonstration of trophozoites in urine, vaginal secretions, cervical secretions, cervical swabs in wet mounts MOTILITY PATTERN: Wobbling or rotary, jerky motility STAINS USED IN MX: Giemsa Papanicolau Romanowsky Acridine orange CULTURE: Diamond’s Modified Medium Feinberg-Whittington Culture Medium Bushley’s CM Roiron’s and Johnson-Trussel CM CPLM ( Cysteine Peptone Liver Maltose) Medium TREATMENT • Both partners must be treated simultaneously and abstain until treatment is finished, otherwise they will be continuously re-infecting each other causing the “Ping-pong effect” • Metronidazole • Tinidazole • Nimorazole • Ordinazole EPIDEMIOLOGY • Worldwide in distribution • Most commonly acquired STD • Prevalence is higher in women of child-bearing age • Higher prevalence with greater frequency of sexual intercourse with multiple sexual partners PREVENTION AND CONTROL • Sexual abstinence • Safe sex • Monogamy ______________________________________________ Trichomonas hominis • Pentatrichomonas hominis • Tetratrichomonas hominis • Trrichomonas intestinalis • Non-pathogenic; commensal only • Trophozoite stage only • Passed out in diarrheic stools MODE OF TRANSMISSION • Ingestion of trophozoite from contaminated food and drinks – Presence of this parasite in food and water indicates fecal contamination HABITAT Cecum (large intestine) DIAGNOSIS • Demonstration of trophozoite in stools • Motility pattern: rapid jerky motility
- 4. TROPHOZOITE Pyriform shape Length: 5-14 um 5 anterior flagella plus a posterior flagellum projecting from the undulating membrane Cytostome situated anteriorly opposite to the Single nuclei situated anteriorly Axostyle extends from the anterior to posterior along the midaxis Undulating membrane** extends all the way through the entire body of the parasite and is free trailing at the posterior end LIFE CYCLE • Ingestion of trophozoite from contaminated food and watertrophozoite in the stomachSIcecum (large intestine) trophozoite replicatespassed out in stool ingested by host EPIDEMIOLOGY • Prevalence in the Philippines is <1% ______________________________________________ Trichomonas tenax • Trophozoite stage only • Non-pathogenic; harmless commensal of the oral cavity • Multiplies by longitudinal binary fission • Can survive for several hours in drinking water HABITAT • Oral cavity MODE OF TRANSMISSION • Kissing • Use of common eating and drinking utensils • Droplet spray from the mouth PREVENTION: good oral hygiene DIAGNOSIS: swabbing the tartar between the teeth, gingival margin, or the tonsillar cryptswet mount or stained slides TROPHOZOITE • Pyriform in shape • Length: 5-12 um (smaller and more slender than T. vaginalis) • 4 flagella plus a 5th one in the margin of the udulating membrane which doesn’t reach the posterior end of the body • Single nuclei and cytostome • Undulating membrane** extends ½ to 2/3 of the body of the parasite ______________________________________________ Chilomastix mesnili • Non-pathogenic; harmless commensal • Indicator of fecal contamination of food and water • Prevalence in the Phils. Is <1% • Treatment is not necessary HABITAT • Cecum (large intestine) MODE OF TRANSMISSION • Ingestion of cysts from contaminated food and water DIAGNOSIS: • Demonstration of trophozoites and cysts in stools PREVENTION • Proper sanitation and personal hygiene TROPHOZOITE • Length: 6-10 um • Assymetrical pear-shaped due to the **spiral groove running obliquely across the ventral surface • Single spherical nucleus with a centrally located karyosome and achromatic fibrils • 3-4 anterior flagella arising from the blepharoplasts and a more delicate one within the prominent cytostome • Cleft-shaped cytostome extends ½ of its body length • Motility pattern: boring progressive motility with slow rotation of the body CYST • Lemon-shaped with nipple-like** or knob-like protuberance • Length: 6-10 um • Single nucleus with centrally located karyosome
- 5. • Cytostome extends throughout the body of the parasite • Cytostomal fibril has a **“Shepherd’s crook” appearance LIFE CYCLE • Ingestion of cyst from contaminated food and watercyst in the stomachSIcecum (large intestine)excystation trophozoite replicates undergoes encystation trophozoite and cyst passed out in stool cyst ingested by host ______________________________________________ Retortamonas intestinalis • Retortamonas intestinalis is a small flagellate and is rarely encountered. • found in both warm and temperate climates • non-pathogenic; harmless commensal • Indication of fecal contamination MODE OF TRANSMISSION • Ingestion of cyst from contaminated food and water HABITAT • Cecum LABORATORY DIAGNOSIS • Demonstration of cyst and trophozoite from stools TROPHOZOITE • The trophozoite is small • Large single nucleus at the anterior portion with small compact karyosome • Length: 4 – 9 um. • Motility: jerky and rotational • 2 anterior flagella and a prominent cytosome that can be seen in an unstained preparation CYST • The cysts are small and pear shaped. • Length: 4-7 um with • 1 large nucleus frequently near the centre. • The fibril arrangement: “birds beak”. LIFE CYCLE • Ingestion of cyst from contaminated food and watercyst in the stomachSIcecum (large intestine)excystation trophozoite replicates undergoes encystation passed out in stool cyst ingested by host