Downloaded 142 times




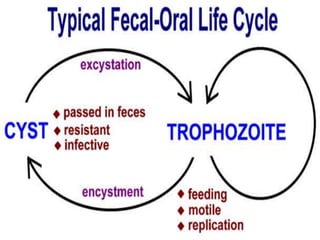

























































This document summarizes gastrointestinal protozoal infections. It discusses various protozoa including Entamoeba histolytica, Giardia lamblia, Cryptosporidium parvum, Balantidium coli, and Isospora belli. It covers the morphology, life cycles, clinical manifestations, diagnosis, and treatment of these protozoa. Risk factors for infection include developing countries, poor sanitation, homosexuality, and immunocompromised states like HIV/AIDS. Protozoal infections commonly cause diarrhea but can also lead to more severe complications in vulnerable groups. Diagnosis involves microscopic examination of stool samples, and treatment consists of antimicrobial agents like metronidazole and nitazox






















































































