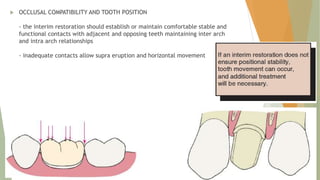
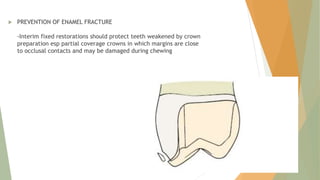
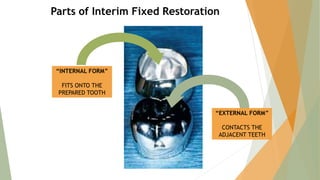
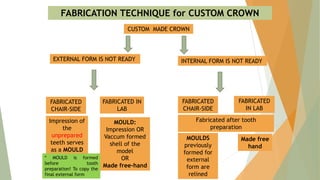
This document discusses interim fixed dental prostheses. Interim restorations are designed to enhance esthetics, stabilization, and function for a limited period of time until being replaced by a definitive restoration. They must satisfy the biological, mechanical, and esthetic needs of the patient and dentist. Interim restorations can be fabricated using direct, indirect, or indirect-direct techniques with materials like acrylic, bis-acryl composites, or preformed shells that are relined. Proper fitting, occlusal compatibility, and marginal adaptation are important to prevent complications before definitive treatment begins.
































































































![Temporization or provisional restoration copy [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/temporizationorprovisionalrestoration-copyautosaved-211029145754-thumbnail.jpg?width=640&height=640&fit=bounds)


































