• Introduction
• Requirementsfor fixed provisional restorations
Provisional luting materials
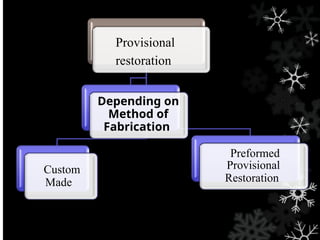
• Types of provisional restorations
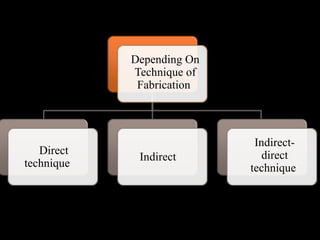
• Various techniques of fabrication:
a.Direct fabrication techniques
b.Indirect method
c.direct- indirect
• Management of provisional restoration short comings
• Summary
• Refrences
3.
INTRODUCTION
• Provisional restorationsin fixed prosthodontic
rehabilitation are important treatment
procedures, particularly if the restorations are
expected to function for extended periods of
time or when additional therapy is required
before completion of the rehabilitation.
• these materials should not only satisfy the
mechanical requirements such as strength and
resistance to wear but also meet the biologic and
esthetic demands.
4.
• Fabrication ofthis definitive prosthesis, on an
average takes about 7-10 days during which the
prepared tooth need to be protected from the oral
environment and also its relationship with the
adjacent and opposing tooth need to be
maintained.
• Thus, in order to protect these prepared teeth,
provisional restorations are fabricated and the
process is called as Temporization .
• The terms provisional, interim, or transitional
have also been routinely used interchangeably
5.
Provisional prosthesis: afixed or removable dental
prosthesis, or maxillofacial prosthesis designed to
enhance esthetics, stabilization, and/or function for
a limited period of time, after which it is to be
replaced by a definitive dental or maxillofacial
prosthesis; often such prostheses are used to assist
in determination of the therapeutic effectiveness of
a specific treatment plan or the form and function
of the planned definitive prosthesis
6.
(Fredrick and
Krug)
• Protectpulpal tissue and sedate prepared
abutments
• Protect teeth from dental caries
• Provide comfort and function
• Evaluate parallelism of abutments
• Provide method for immediately replacing
missing teeth
• Prevent migration of abutments
• Improve esthetics
• Evaluate and reinforce the patient’s oral home
care
Rationale for Provisionalrestorations
7.
• Provide amatrix for the retention of periodontal
surgical dressings
• Stabilize mobile teeth during periodontal
therapy and evaluation.
• Provide anchorage for orthodontic brackets
during tooth movement
• Aid in developing and evaluating an occlusal
scheme before definitive treatment
• Allow evaluation of vertical dimension,
phonetics, and masticatory function
• Assist in determining the prognosis of
questionable abutments during prosthodontic
treatment planning
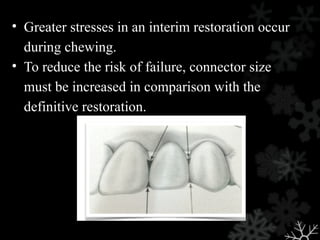
• Greater stressesin an interim restoration occur
during chewing.
• To reduce the risk of failure, connector size
must be increased in comparison with the
definitive restoration.
10.
Indications of provisionalrestorations
• Diagnostic: Prior to making the final restoration it
may be advisable to determine the prognosis of the
pulps and the periodontium of the prepared tooth.
• Protective: Cut dentine and associated pulp are
protected from salivary, thermal and chemical
irritants. The gingival is also protected when
restorations are properly formed
• Restorative: Replacement of teeth, especially
immediate anterior replacements.
11.
• Restorative: Replacementof teeth, especially
immediate anterior replacements.
• Stabilization or Provisional Splinting: Stabilization
is of great importance in the treatment of
periodontal weakened teeth. this type of temporary
restoration acts as a provisional splint
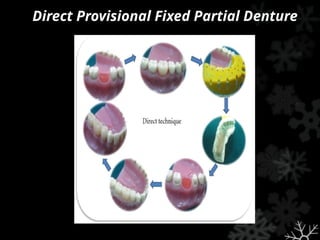
Direct Provisional FixedPartial Denture
• For urgent situations, in the absence of any
matrix or opportunity to create a matrix, a
provisional restoration can be fabricated by
adapting a block of freshly mixed
acrylic resin directly to a tooth.
• After the acrylic resin block has polymerized,
the tooth contours can be carved with burs
of choice and the restorative margins perfected
intraorally.
17.
Direct Provisional FixedPartial Denture
Advantage :
- Less time consuming as the intermediate steps of
indirect technique are eliminated.
Disadvantages :
- Potential tissue trauma from the polymerizing
resin, and
- Inherently poor marginal fit.
• Indirect: theseare constructed by placing the
matrix over a model of the prepared tooth, thus
the provisional is constructed out of the
patient's mouth.
• Advantages:
1.No contact of monomer with the prepared tooth or
gingiva.
2.Avoids subjecting a prepared tooth from the heat
created from polymerization.
3.Marginal fit is better.
4.Comfortable to the patient.
21.
• Indirect-Direct: Theseare made by forming
a temporary in an indirect manner and
then relining this directly in the patients mouth.
• Advantage:
1.Chair side time is reduced.
2.Less heat generated in mouth.
3.Contact between the resin monomer and soft
tissue is minimised.
22.
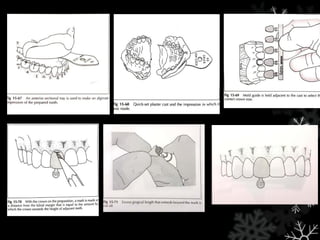
Over impression fabricatedprovisional crown
• Over impression frequently is made in the
patient mouth while waiting for the anesthetic
to take effect
• If the tooth to be restored has any obvious
defect , the over impression should be made
from the diagnostic cast
• Any defect can be filled with utility wax
24.
• When thealginate has set the over impression
can be removed from the diagnostic cast
• Thin flashes of impression material that
replicate the gingival crevice are
removed to insure that there will be no
impediments to the complete seating of the cast
into the overimpression later
25.
• The impressionis wrapped in a wet paper towel
and placed in a zip lock plastic bag for later use.
• When the tooth preparation is completed, another
quadrant impression is made in alginate. This
impression is poured up with a thin mix of
quicksetting plaster .
26.
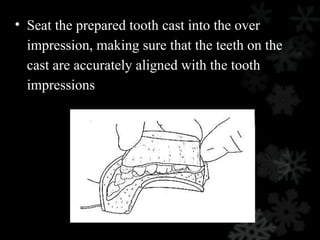
• Seat theprepared tooth cast into the over
impression, making sure that the teeth on the
cast are accurately aligned with the tooth
impressions
27.
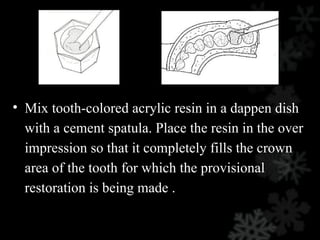
• Mix tooth-coloredacrylic resin in a dappen dish
with a cement spatula. Place the resin in the over
impression so that it completely fills the crown
area of the tooth for which the provisional
restoration is being made .
28.
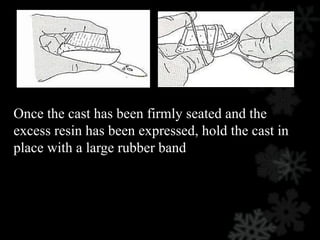
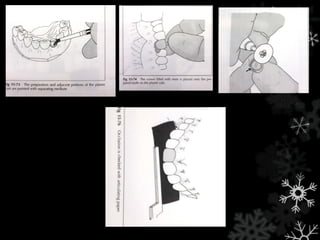
Once the casthas been firmly seated and the
excess resin has been expressed, hold the cast in
place with a large rubber band
29.
• It isimportant that the cast be oriented securely in
an upright position so that the space between the
cast and the impression that is filled with the resin
forming the provisional restoration will not be
distorted.
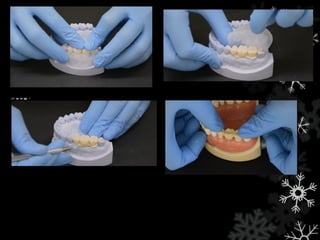
Template fabricated VLCprovisional restoration
• A transparent template is essential to the use of a
visible light cured resin
• Template is filled with light cured resin.Use firm
pressure to seat the loaded template on the quick
set plaster cast
• Cast with resin loaded template is placed on the
light polymerising unit
• Remove from polymerising unit, trim excess with
scissors Finishing and polishing
34.
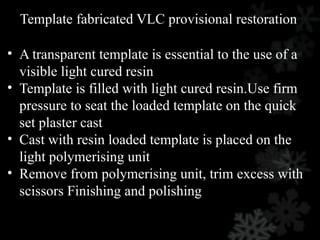
Over impression fabricatedbisacryl composite
Impression of the sextant taken
A gingival trough is cut With
no 8 bur in facial and lingual
surfaces of imprint of tooth
being restored
Mixed resin is expressed into the Imprint of the tooth for
which provisonal Restoration s being fabricated
35.
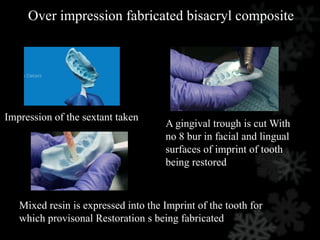
Tease the restoration
Positionthe impression tray on the tooth ,
App. 2min
Remove excess near the margin
When elastic , can remove, shouldn’t take
more than 6 min from mixing
36.
Shell fabricated provisionalcrown
• A thin shell crown or fpd can be made from
any acrylic resin , and then that shell can be
relined indirectly or directly in the mouth .
• If the reline is done directly ,a methacrylate
other than polymethyl should be used
• This technique can save your chair because the
restoration is partially fabricated prior to the
preparation appointment
37.
An overimpression ismade from diagnostic wax up
With an insufflator gently spray enough polymer on to surface of
impression to absorb monomer.
Trim of excess flash material created by the gingival
crevice
Use plastic squeeze bottle with a fine tip to deposit one drop on the
lingual surface of the imprint of each tooth to be restored.
Keep the monomer near the gingival portion of the impression to
prevent excess from accumulating in the incisal or occlusal surface
38.
Try shell onthe cast
Gently remove shell from the impression after 4 min
Teeth have been prepared, make a quandrant alginate and pour
with quick setting plaster.
Repeat the process 4 times , inverting the impression frequently to allow the
material to run down to margin rather than pudding in incsial or occlusal
surface
Trim the flash from the gingival area and open the gingival
embrasure with an abrasive disc
39.
Trim the excess
Seatthe shell onto the prepared teeth on the cast
When the resin has polymerised, remove the band and dissemble
the shell from plaster
Monomer and polymer can be added directly to shell and mixed there or
mixed in a dappen dish and then transferred to shell , completely filling each
tooth
Wrap a rubber around the shell and cast and place them in a
plaster bowl full of hot tap water for approximately 5mi
40.
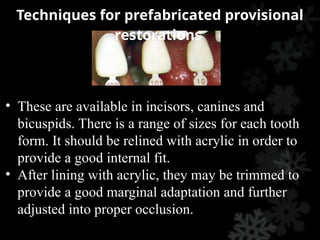
• These areavailable in incisors, canines and
bicuspids. There is a range of sizes for each tooth
form. It should be relined with acrylic in order to
provide a good internal fit.
• After lining with acrylic, they may be trimmed to
provide a good marginal adaptation and further
adjusted into proper occlusion.
Techniques for prefabricated provisional
restorations
45.
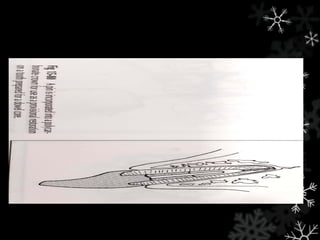
PROVISIONAL CROWN FORAN
ENDODONTICALLY TREATED TOOTH
• It is often difficult to fabricate provisional
restoration for a tooth that has been prepared for a
dowel core because there is so little intact
supragingival tooth structure.
• This can be accommodated for in the use of
standard polycarbontae crown by placing a piece
of paper clip or other stiff wire into canal and
place resin filled crown down over that.
47.
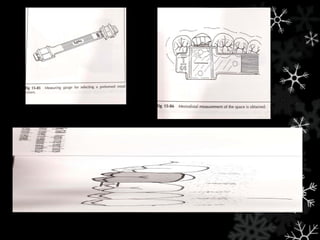
PREFORMED ANATOMIC METALLICCROWN
• Emergency cases involving fractured molars
are one of the best indication for the use of
preformed metal crown.
48.
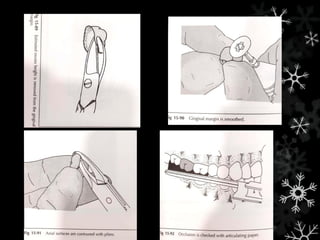
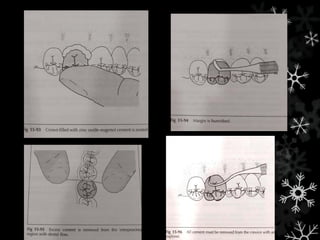
Procedure consist of
•minimal tooth preparation
• measurement and selection of crown
• trimming and adaptation of gingival margin
• occlusal adjustment
• cementation
53.
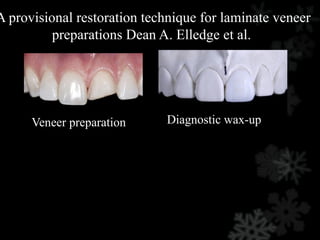
• Porcelain veneersare a very conservative
treatment for changing the shape, shade, and
contour of teeth without resorting to full-
coverage restorations. These restorations rely
upon the bond between enamel and the porcelain
veneer.
• Fabrication of provisional restorations for
veneers can be a time-consuming and difficult
task. The minimal reduction typically done and
fragility of the thin temporaries make the
process even more challenging.
54.
A provisional restorationtechnique for laminate veneer
preparations Dean A. Elledge et al.
Veneer preparation Diagnostic wax-up
55.
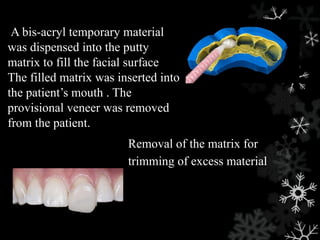
Removal of thematrix for
trimming of excess material
A bis-acryl temporary material
was dispensed into the putty
matrix to fill the facial surface
The filled matrix was inserted into
the patient’s mouth . The
provisional veneer was removed
from the patient.
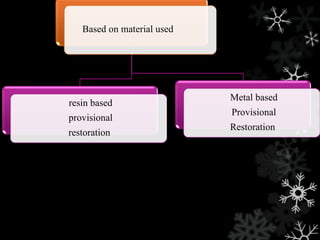
Acrylics: since 1930sthe most commonly used
materials today for both single-unit and multiple-
unit restorations
• They produce acceptable short-term
provisionals but tend to discolour over time.
• disadvantages : objectionable odour,
significant shrinkage and heat generation
during setting.
MATERIALS USED IN THE FABRICATION OF
PROVISIONAL CROWNS
• Polymethyl methacrylatesare commercially
available as
Jet (Lang),
Alike (GC America),
Temporary Bridge Resin (Dentsply/Caulk),
Neopar (SDS/Kerr),
Duralay (Reliance)
60.
• Advantages ofthis material include low cost, good
wear resistance, good esthetics, high polishability,
good colour stability
• Drawback : It warps because of polymerization
shrinkage
• Heat production during polymerization due to the
exothermic reaction which can damage pulp
• The free monomer that is present may cause pulpal
and gingival damage
61.
• Plant etal. found that the intra-pulpal temperature
rise associated with the polymerization of methyl
methacrylate materials could be up to five times
that associated with the normal consumption of
thermally hot liquid
Plant CG, Jones DW, Darvell BW. The heat evolved and temperatures attained during
setting of restorative materials. Br Dent J 1974;137:233-8.
62.
Poly-R' Methacrylates -Snap ,Splintline ,Trim
II ,Provisional C&B Resin and Temp Plus
• advantages like low cost, less heat given off
during reaction, less shrinkage than polymethyl
methacrylates and extended working time
• disadvantages which include less esthetic than
other currently marketed materials, eugenol
deteriorates the resin, poor wear resistance, poor
colour stability, objectionable odour, hard to
repair and radiolucent.
63.
• Epimines werethe first two-paste acrylics,
commercially introduced in 1968 as Scutan
(ESPE). Although Scutan had relatively low
shrinkage, heat production and lowest pulpal
irritability, it was weak and could not be
altered or repaired.
64.
• Preformed provisionalcrowns or matrices
usually consist of tooth-shaped shells of
plastic, cellulose acetate or metal.
Polycarbonate crowns
First described by Charles et al in 1973.
•Most natural appearance
•Advantages:
1.Esthetics
2.Readily available
3.Save chair-side time
65.
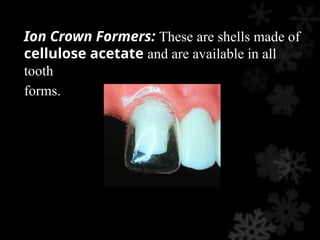
Ion Crown Formers:These are shells made of
cellulose acetate and are available in all
tooth
forms.
66.
• These shellscome in various sizes for each
tooth form and are lined with acrylic resin.
After the acrylic resin has polymerized, the
cellulose shell is peeled away from the
crown.
• This usually necessitates the further addition of
acrylic in the areas of the proximal contacts.
67.
• Aluminium crownforms
1.These have been used for many years as the
material is easy to manipulate, and it is malleable
and ductile.
2.Aluminium crown forms can corrode with time as
saliva can react with them.
3.There is also a risk that if they are placed adjacent
to a freshly packed amalgam or gold restoration, a
galvanic cell may be established.
68.
Stainless steel crownforms:
1. These crown forms are much less malleable and
ductile than the aluminium crown forms, thus they
are harder wearing and are less likely to deform
under load.
2. They are usually not refined but trimmed using
crown shears until their fit approximates to the
prepared tooth and luted using a glass ionomer or
polycarboxylate cement.
3. The success rate is very high and these crowns
are useful to maintain the space that may be lost
when a deciduous tooth is lost prematurely.
69.
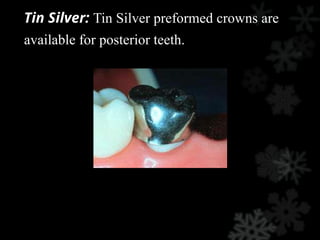
Tin Silver: TinSilver preformed crowns are
available for posterior teeth.
70.
• This alloyis very soft and the margin
of the crown can be flexed prior to
seating.
• This produces a close marginal fit after
the shell is trimmed with a bur.
• These should also be lined with nacrylic
resin to provide good internal
adaptation and retention of the temporary.
71.
• Nickel chromiumalloy:
1.Used in children with extensively damaged
primary teeth
2.They cannot be altered with resin
3.These crowns can be easily recontoured using
pliers.
4.Indicated as long term temporaries.
72.
Composites :auto-polymerized, dualpolymerized
andvisible light polymerized
• shrink less, give off less heat during setting,
• excellent esthetics, minimal odor and can be
polished at chair-side.
• Protemp II, Protemp Garant, Protemp IV,
Provitec
• For bothanterior and posterior teeth, they
found the bis-acryl materials significantly
superior to PMMA in all categories and
amongst the various materials, studies have
concluded that Protemp IV is most colour
stable and with superior mechanical
properties.
75.
Protemp™ Crowns (3MESPE)
A Bis-GMA light-cured composite
• Have a single shade only,
• Have good wear resistance
• Good polishability,
• But because of their single shade are somewhat
limited unless one is prepared to custom stain
76.
Luxatemp Ultra
• Incorporatingproprietary nano technology
• Luxatemp Ultra surpasses all leading provisional
materials in flexural strength
77.
CAD-CAM PMMA Provisonals
•Provisional restorations are digitally fabricated
from polymethyl methacrylate (PMMA) and
yeilds a highly precise and anatomically detailed
result .
• PMMA temporaries are milled out of a dense
block and shows reduced the porosity of
traditional hand processed techniques, reducing
chair time and cracking.
• Axial contours and occlusal anatomy provided
from tooth libraries produce additional anatomy
that mimics natural teeth
78.
BioTemps provisionals
Indicated forprovisional splinted crowns and
provisionalfull-arch bridges. BioTemps Implant
Provisionals looks like realistic temporaries at any
stage of implant treatment.Cast-metal substructure
is indicated when pontic span is greater than 3
units. BioTemps with metal reinforcement last up
to six months.
79.
There are avariety of luting materials used for
interim purposes. The most common include
(1) polycarboxylate
(2) zinc-oxide eugenol
(3) non-eugenol materials.
80.
• The retentiverequirements for provisional luting
materials are that they be: strong enough to retain
a provisional restoration during the course of
treatment but,allow easy restoration removal when
required.
• This paradoxical necessity for good retentive and
sealing quality and easy restoration retrieval may
lead to a compromise in material behavior,
particularly regarding mechanical properties.
81.
• Baldissara etal recommended that interim
restorations be frequently evaluated and used
for only short periods of time.
• Literature reports advise that if provisional
treatment is required over a protracted time
period, it is best to remove and replace the
provisional luting agent on a regular basis
82.
• Some ofthe most commonly used cements with
provisional prostheses are those containing zinc-
oxide and eugenol. They provide:
sedative effects to reduce dentin
hypersensitivity
possess antibacterial properties.
83.
• Eugenol interfereswith the acrylic resin
polymerization and hardening process .
• Therefore Eugenol-free provisional luting
materials are commercially available and
have gained popularity due to the absence of
resin-softening characteristics .
ZONE TEMPORARY LUTINGCEMENTS
• Replace eugenol with various types of
Carboxylic acids.
• Compatible with permanent resin cements.
• Greater retention than ZOE cements.
• No Sedative effect on pulp.
• ex. Rely X Temp NE(3M ESPE), Temp Bond
NE (Kerr), Freegeno
MANAGEMENT OF PROVISIONAL
RESTORATIONSHORTCOMINGS
Fracture
s
• upon removal from the mouth, during
construction trimming, or function.
• result of a crack propagating from a surface
flaw,
• It alters transverse strength, impact
strength, and fatigue resistance
88.
method to reducethe likelihood of fracture
• select the appropriate material based on its
behavior in the oral environment when it will be
subject to aging, fatigue, water sorption, and
wear processes
• it is important to know the flexural strength of
various types of resins for provisional
restorations, as most of them are brittle
• it is generally accepted that PMMAs exhibit
higher fracture toughness than bisphenol A
glycidyl methacrylate (bis-GMA) resins
89.
Non-integrity of theExternal Contour:
• The correct shaping of the external contours
provides proximal and occlusal stability, and
• maintains tooth positions while the restorative
plan is executed.
90.
Marginal Inaccuracy:
• shouldexhibit accurate marginal adaptation to the
finish line of the prepared tooth in order to protect
the pulp from thermal, bacterial, and chemical
insults.
• Deficiencies can occur when auto-polymerizing
acrylic resin is used, due to dimensional
contraction
• the resulting marginal gaps may be minimized by
relining the restorations
91.
• Relining hasbeen recommended at the time of
fabrication in order to compensate for the
polymerization shrinkage of the resin and to
improve the initial retention
92.
REMOVAL OF PROVISIONAL
RESTORATION
•The provisional is removed when the patient
returns for the definitive restoration or for
continued preparation.
• Risk of damage to the prepared tooth can be
minimized if removal forces are directed parallel
to the long axis of the preparation.
• The Backhans or hemostatic forceps are
effective.
• Slight buccolingual rocking motion will help
break the cement seal.
93.
CONCLUSION
Although provisional restorationsare usually
intended for short term use and then discarded, they
can be made to provide pleasing esthetics, adequate
support, and good protection for teeth while
maintaining periodontal health.
94.
They may befabricated in the dental office or in
laboratory from any of several commercially
available materials and by a number of practical
methods.

























![Temporization or provisional restoration copy [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/temporizationorprovisionalrestoration-copyautosaved-211029145754-thumbnail.jpg?width=640&height=640&fit=bounds)






















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






