Downloaded 110 times
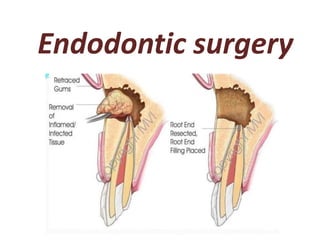
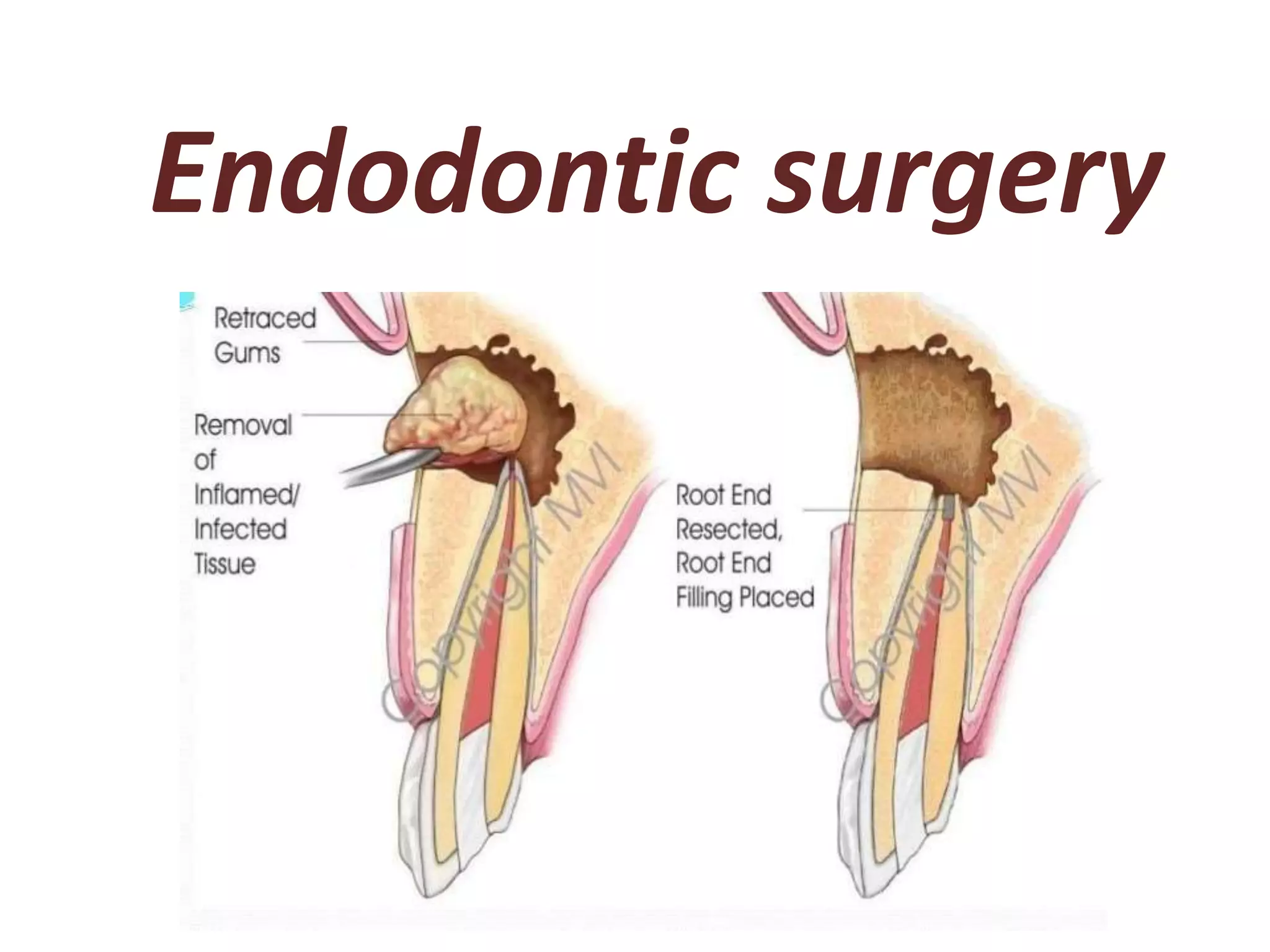
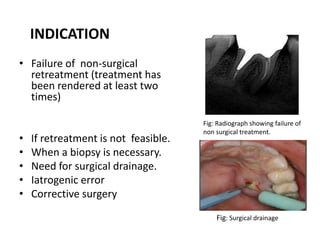
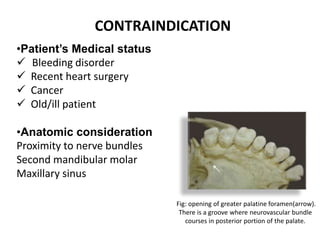
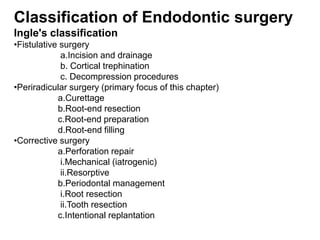
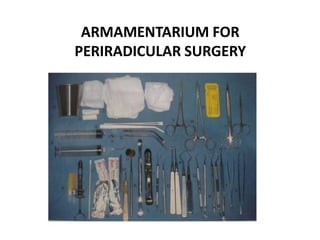
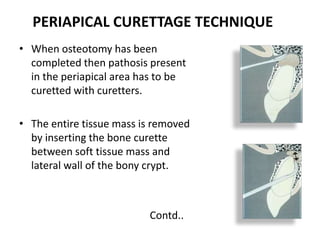
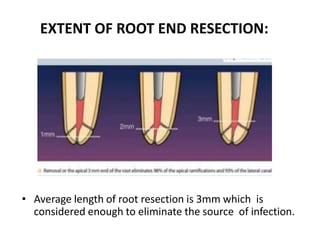
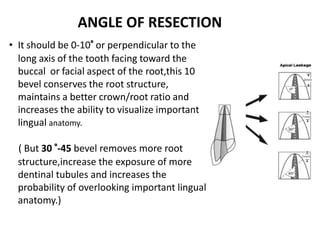
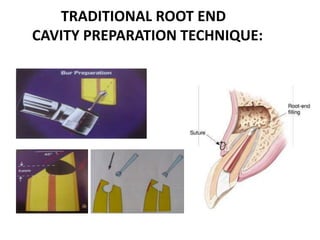

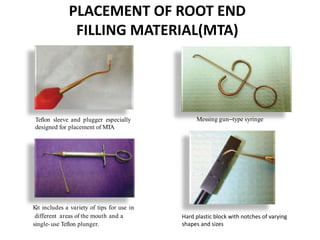





The document discusses endodontic surgery, including: - Indications for endodontic surgery when non-surgical retreatment has failed or is not feasible. - Classification, armamentarium, treatment planning considerations, and stages of surgical endodontics including flap design, osteotomy, periradicular curettage, root-end resection, and root-end preparation and filling. - Key aspects are proper anesthesia, hemostasis, management of soft and hard tissues to access the surgical site and root structure for periradicular procedures.


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)