INTRODUCTION
• For manyyears the management of vestibular schwannoma
did ,in fact,nearly always mean surgical management.The main
reason for this was late diagnosis.
• Most vestibular schwannomas originate in the region of the
Internal Acoustic Meatus(IAC), enlarging the porus and
extending into cerebellopontine angle (CPA)
3.
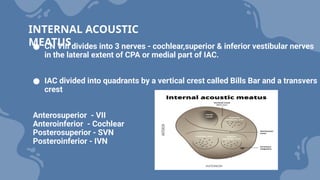
● CN VIIIdivides into 3 nerves - cochlear,superior & inferior vestibular nerves
in the lateral extent of CPA or medial part of IAC.
● IAC divided into quadrants by a vertical crest called Bills Bar and a transvers
crest
Anterosuperior - VII
Anteroinferior - Cochlear
Posterosuperior - SVN
Posteroinferior - IVN
INTERNAL ACOUSTIC
MEATUS
4.
● it remainsunclear whether it was Ballance in London or
Annandale in Edinburgh who performed the first
successful VS removal
● these operations were carried out through the suboccipital
approach
● William House in the 1960s proposed surgery as soon as
the diagnosis could be made and suggested the
translabyrinthineapproach to the CPA.
HISTORY
5.
● logic ofletting a small or medium-sized tumour become a
large or giant tumour before performing an operation that
was almost inevitably bound to be associated with a poor
outcome or even death.
● House endured many hostile confrontations with the
neurosurgical community, whose objections were as much
due to the fact that otologists were becoming involved with
this type of surgery as with the approach itself
This is nowthe favoured approach for the removal of
VS for the majority of neurotologists
Translabyrinthine approach
11.
The key stagesin the operation are:
1. Skin and periosteal flaps
2. Extended cortical mastoidectomy
3. Bony labyrinthectomy
4. Skeletonization of the jugular bulb and vertical portion
of the facial nerve
5. Skeletonization of the IAM
6. Identification of the facial nerve at the lateral end of
the internal meatus
7. Opening of the posterior fossa through the dura of the
posterior surface of the petrous bone
8. Removal of tumour using standard neurosurgical
techniques
9. Closure with obliteration of the middle ear and petrosectomy
defect, usually with abdominal fat.
12.
● The patientis placed on the operating table in the supine
position with the head turned 30 degrees away from the
surgeon
● Two-channel neuromonitoring for the facial nerve is usually sufficient,
but with very large tumours it may be necessary to monitor the lower
cranial nerves as well.
● The anaesthetist should be reminded that neuromuscular blocking
agents must not be used after intubation.
DETAILS OF THE TRANSLABYRINTHINE APPROACH
POSITION
13.
● A curvedincision above and behind the pinna is planned,to
allow adequate access for bone removal behind the lateral
sinus and anterior access to the labyrinthine part of the facial
nerve
● For tumours up to about 2.5 cm intracranialdiameter the
incision can be about 3 cm behind the postauricular sulcus
but for larger tumours the incision should be sited further
back to allow exposure of the of the dura behind the lateral
sinus
Skin incision
14.
• It isdesirable to create a separate flap that can be used during
closure to secure the abdominal fat plug
• The flap can be pedicled superiorly or anteriorly
• The superiorly based flap has the advantage that, if necessary,
it can easilybe extended upwards to allow access to the
middle cranial fossa.
Musculoperiostial flap
15.
● Using cuttingand coarse diamond paste burrs, bone is removed up
to the middle fossa dura,exposing it widely, both over the floor of the
middle fossaand some 3–4 cm up the squamous portion of the
temporal bone.
● this allows easy retraction of the dura with the instruments during
tumour removal.
● In a similar manner, bone is removed from the sigmoid sinus and
from the bone overlying the posterior fossa dura for 2–3 cm behind
the sinus.
● The sinus can thus be compressed backwards to increase access
Cortical mastoidectomy
16.
● During preparationof the sigmoid sinus, troublesome
bleeding may be encountered from a large emissary vein. If
possible it is better to anticipate trouble and identify and
control the vein before making it bleed.
● Its bony canal can be skeletonized and obliterated with bone
wax or, alternatively, the vein can be coagulated with bipolar
diathermy.
● Coagulation should not be too close to the main sinus
otherwise the manoeuvre may simply convert a small bleed
from the emissary vein into a large bleed from the sinus.
● Care must be taken to avoid damage to the superior petrosal
sinus, which runs along the posterior petrous ridge
17.
● The bipolardiathermy, if applied lightly over the dura or the
surface of the sigmoid sinus, will make it retract and increase
access.
● Bleeding from the superior petrosal sinus and, indeed, even
from the lateral sinus, is easily controlled with pressure and
the application of haemostatic mesh (Surgicel).
● Attention can now be turned to further bone removal
medially. Ensuring the mastoid tip is removed with exposure
of the digastric ridge, which aids in identification of the
descending facial nerve.
18.
● Fig. 1.Left temporal bone after
mastoidectomy, opening of the facial
recess, removal of the incus, and
decompression of the sigmoid sinus and
middle fossa dura complete. Next steps
include labyrinthectomy, opening of the
IAC and posterior fossa, and dissection of
the tumor from the critical neurovascular
structures. Dashed lines indicate deeper
structures not yet uncovered. FR, Facial
recess; IAC, Internal auditory canal; LSCC,
Lateral semicircular canal; M, Malleus;
PSCC, Posterior semicircular canal; SSCC,
Superior semicircular canal.
19.
● A standardtotal bony labyrinthectomy is performed
● Care must be taken in drilling out the ampulla of the posterior canal,
which lies medial to the second genu of the facial nerve
● The ampulla of the superior semi-circular canal should be retained
as it is a landmark for the superior vestibular nerve –SVN
● In drilling out the superior canal the surgeon will encounter the
subarcuate artery, which runs under the canal and leads to the
posterior fossa dura just behind the porus of the internal meatus.
● The endolymphatic duct can be traced from the vestibule along the
line of the common crus where it turns through 90 degrees towards
the posterior fossa dura and widens out to become the sac.
Bony labyrinthectomy
20.
● The boneover the posterior fossa dura between the labyrinth
and the anterior margin of the sigmoid sinus should be
removed and access is further enhanced, especially in small
temporal bone, if bone is progressively removed from the
dura of the middle fossa.
• It is by removing these bony boundaries of the petrous bone
so that the limits of the resection are the soft and
compressible dural surfaces that the surgeon gets maximum
access to the posterior fossa
• This is one of the secrets of success in the translabyrinthine
operation.
• Although opening of the labyrinth almost inevitably leads to
total hearing
21.
● there havebeen attempts to perform a conservative
labyrinthectomy with sealing of the vestibule and thus
isolation of the cochlea from the labyrinth with preservation
of the hearing.
● This technique was first described by McElveen et al.2
● Currently in attempting cochlear nerve preservation, a three-
channel intracochlear electrode is inserted during the latter
stages of the approach and tumour dissection to allow
monitoring of the cochlear nerve function.
22.
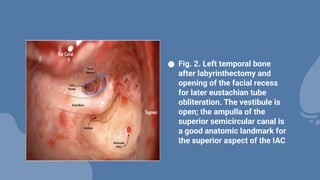
● Fig. 2.Left temporal bone
after labyrinthectomy and
opening of the facial recess
for later eustachian tube
obliteration. The vestibule is
open; the ampulla of the
superior semicircular canal is
a good anatomic landmark for
the superior aspect of the IAC
23.
● The jugularbulb is the lower limit of bone removal and in nearly all
cases bone should be removed down to its level.
● The height of the bulb does vary enormously. In some very large,
well pneumatized temporal bones with a low bulb and a small
tumour it may not be absolutely necessary to expose the bulb.
● On the other hand it is not at all uncommon for the dome of the bulb
to rise up to, and beyond, the level of the floor of the internal
meatus, even as high as the middle fossa dura, and in these cases
the surgeon must be prepared to mobilize and depress it.
Skeletonization of the jugular bulb and the vertical
portion of the facial nerve
24.
● This isdone by gently freeing the bulb from its bony bed and
packing it downwards using haemostatic mesh (Surgicel) and
bone wax. Bleeding, sometimes quite brisk, may occur but it
is usually easy to control.
● The retrofacial air cells are exenterated and bone may be
removed over the vertical portion of the facial nerve until the
sheath is visible through the bone.
● The exact extent of bone removal over the nerve depends on
the access in the individual temporal bone and the size of the
tumour.
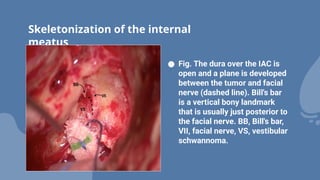
25.
Skeletonization of theinternal
meatus
● Fig. The dura over the IAC is
open and a plane is developed
between the tumor and facial
nerve (dashed line). Bill's bar
is a vertical bony landmark
that is usually just posterior to
the facial nerve. BB, Bill's bar,
VII, facial nerve, VS, vestibular
schwannoma.
26.
● The facialnerve is displaced from its normal position by the
tumour
● It runs along the anterosuperior quadrant of the meatus as far
as the porus where it is displaced to a variable extent anteriorly
and/or superiorly
● before turning down over the front of the tumour to the
brainstem, which it joins just above the pontomedullary
junction.
● Thus in the translabyrinthine approach the tumour is usually
Identification of the facial
nerve
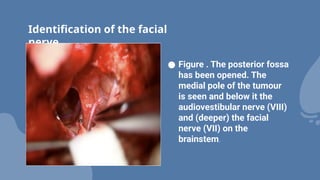
27.
Identification of thefacial
nerve
● Figure . The posterior fossa
has been opened. The
medial pole of the tumour
is seen and below it the
audiovestibular nerve (VIII)
and (deeper) the facial
nerve (VII) on the
brainstem.
28.
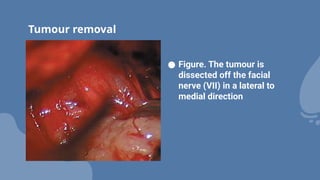
Tumour removal
● Figure.The tumour is
dissected off the facial
nerve (VII) in a lateral to
medial direction
29.
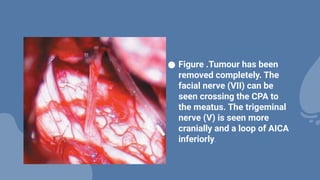
● Figure .Tumourhas been
removed completely. The
facial nerve (VII) can be
seen crossing the CPA to
the meatus. The trigeminal
nerve (V) is seen more
cranially and a loop of AICA
inferiorly.
30.
● This isone of the most important steps in the translabyrinthine
operation.
● CSF fistula remains one of the most common post-operative
problems
● To minimize the risk, careful obliteration of the middle ear and
the temporal bone defect is essential.
● Harvest of free autologous fat (and fascia) from the abdominal
wall or thigh is performed and prepared for use.
● The incus is removed and a posterior tympanotomy created.
● The middle ear, Eustachian tube and vestibule are obliterated
with muscle or fascia and bone wax.
Closure
31.
● The supraand inframeatal gutters are obliterated with fat and obvious
air cell tracts sealed with bone wax.
● The temporal bone defect is obliterated with abdominal fat either in
strips or in one large piece.
● Some surgeons first seal off the posterior fossa and drilled anterior
surface of the petrous bone with fascia lata from the thigh or fascia
from the superficial layer of the external oblique from the anterior
abdominal wall.
● The repair is secured with fibrin glue, although excessive reliance on
biological glues is to be regarded with caution. It is possible that they
may interfere with the body’s natural healing response and, when they
are absorbed, actually predispose to CSF fistula
32.
● The periostealflap is then sutured back over the fat and the
skin closed in two layers.
● A firm pressure dressing is applied and kept in place for a
week.
● It should not, however, be so tight that it causes pressure
changes in the skin of the forehead.











































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

