Downloaded 392 times
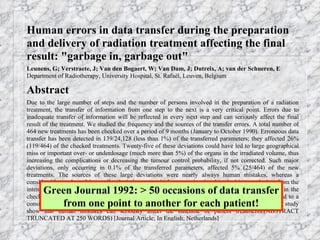
![The impact of patient positioning on the adequate coverage of the uterus in the primary irradiation of cervical carcinoma: a prospective analysis using magnetic resonance imaging. Weiss E et al Radiother. Oncol. 63 (2002) 83 Results : Standard portals [ie 4 field box] did not completely cover the uterus in supine position in 7/21 (33%), in prone position with belly board in 7/21 (33%) and without belly board in 5/21 (24%). Insufficient uterine coverage was found only in the anteroposterior direction. The mean distance (± standard deviation) between the field borders of the lateral portals and the uterus was in supine position anteriorly 3.4 cm (±2.2 cm) and posteriorly 1.8 cm (±1.3 cm), in prone position with belly board anteriorly 2.2 cm (±2.7 cm) and posteriorly 2.6 cm (±1.6 cm), prone without belly board anteriorly 3.3 cm (±2.4 cm) and posteriorly 1.9 cm (±1.1 cm). The difference was statistically significant between supine and prone position with belly board and between prone position with and without belly board. Repeated MRI controls during therapy showed no significant changes compared to the MRIs at the beginning of therapy. Conclusions : The use of standard radiation fields results in a high percentage of geographical misfits. Three-dimensional treatment planning is a prerequisite for adequate uterus coverage.](https://image.slidesharecdn.com/imrtincervixcancer-090531035528-phpapp01/85/Imrt-In-Cervix-Cancer-11-320.jpg)
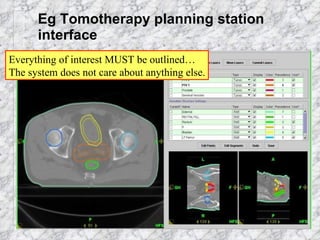
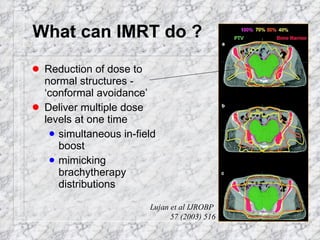
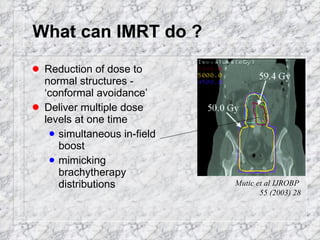
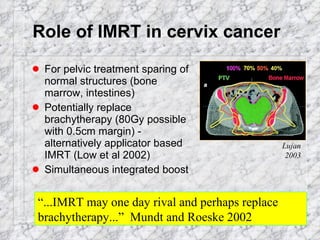
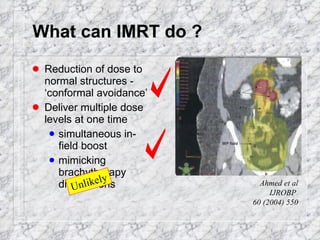

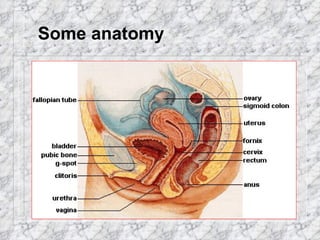
This document discusses the use of intensity-modulated radiation therapy (IMRT) for treating cervix cancer. It notes that IMRT is rarely used currently but could help reduce dose to normal tissues and potentially replace brachytherapy. The document outlines the need for accurate target volume definition using imaging like MRI and CT. It also describes the inverse planning process for IMRT and challenges like organ motion. While IMRT may help spare organs at risk, issues like increased leakage, integral dose and treatment time must be considered.






























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)












