Download as PDF, PPTX
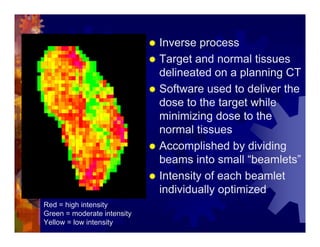
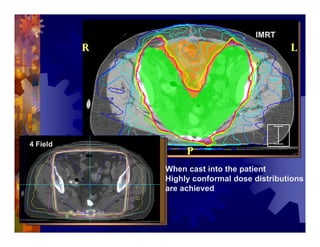

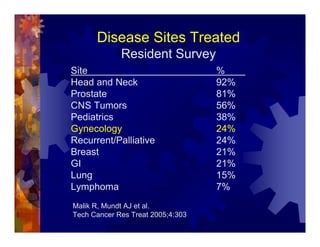
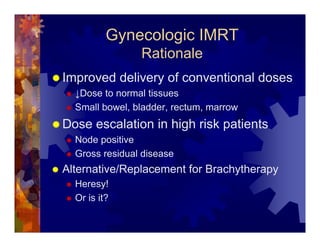
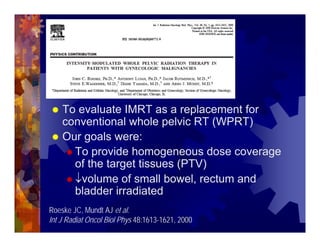

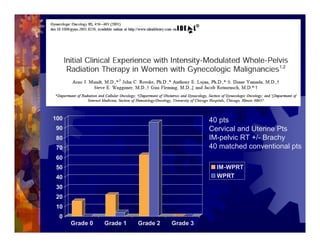
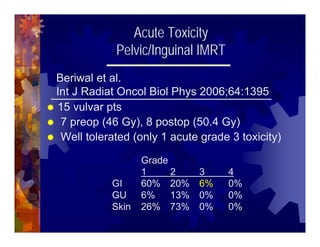
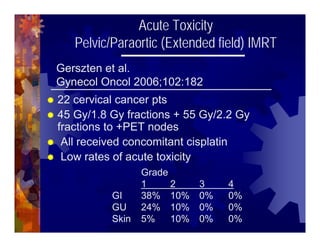






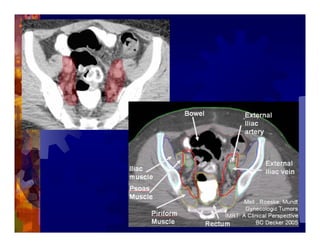




1) Intensity modulated radiation therapy (IMRT) is a technique that uses computer software to conform the radiation dose to the shape of the tumor, reducing dose to surrounding normal tissues and decreasing toxicity. 2) Numerous studies have shown IMRT provides better sparing of the small bowel, bladder, and rectum compared to conventional radiation for gynecologic cancers. 3) IMRT may allow dose escalation to high risk sites or involved nodes while maintaining normal tissue doses. Some studies have also investigated using IMRT as an alternative to brachytherapy boosts. 4) Clinical studies suggest IMRT results in low rates of acute gastrointestinal and genitourinary toxicity compared to conventional radiation for











































































































