Downloaded 313 times
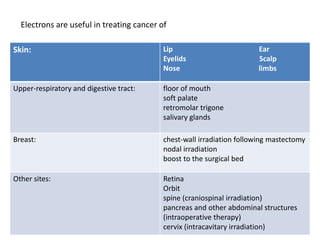
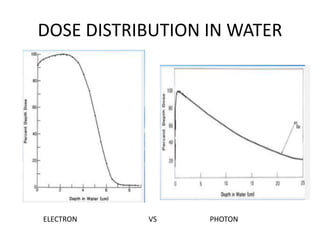
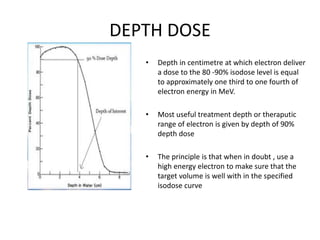





1) Electron beam therapy uses high-energy electrons between 6-20MeV to treat superficial tumors less than 5cm deep. It is useful for cancers of the skin, eye, breast, head and neck, and gastrointestinal tract. 2) Electron beams have distinct advantages over x-rays and brachytherapy in minimizing dose to deeper tissues and providing dose uniformity. 3) The depth that receives 90% of the maximum dose, called R90, is typically one-third to one-fourth of the electron energy in MeV. This determines the maximum treatment depth.











































































