Downloaded 180 times


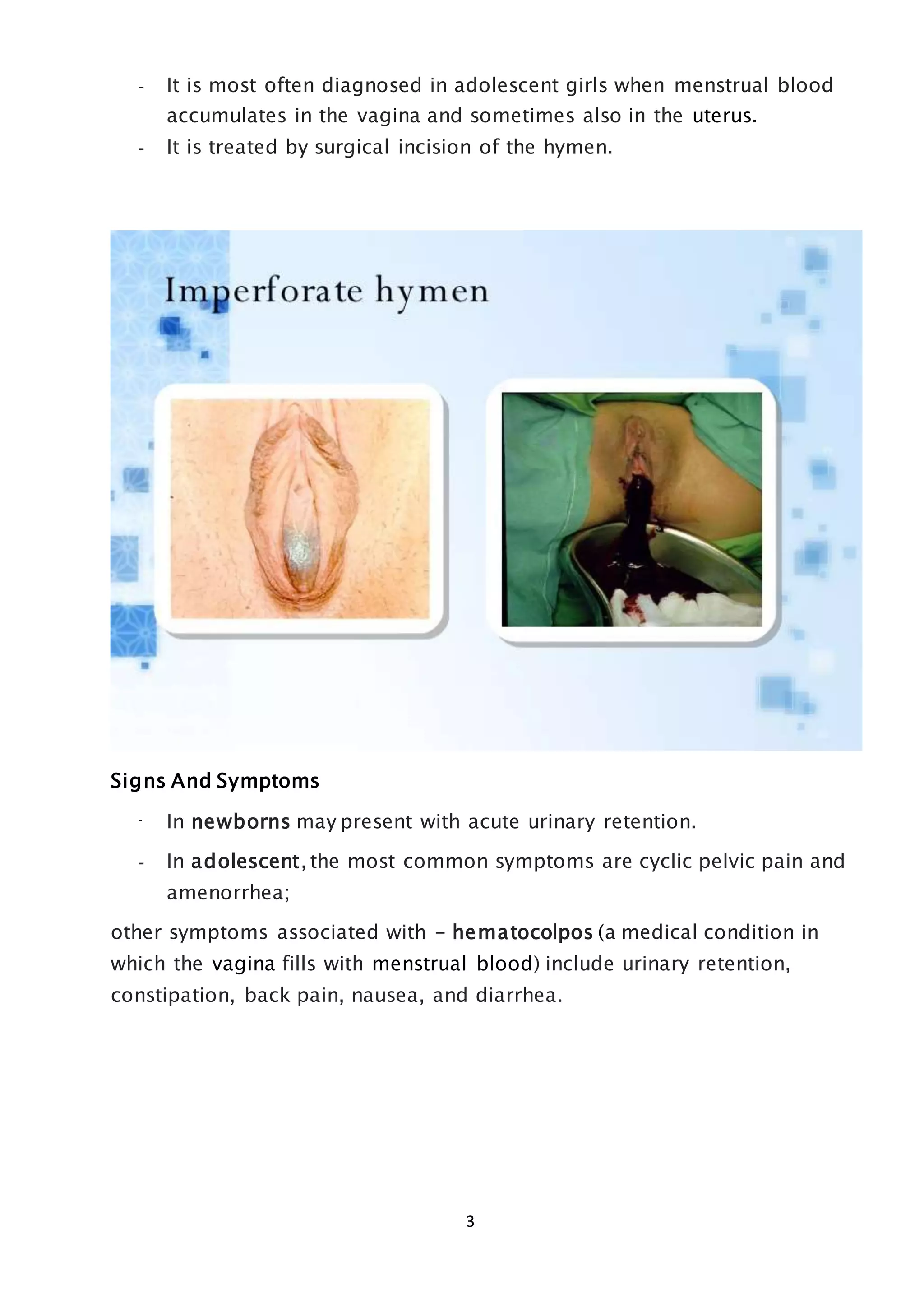


The hymen is a membrane partially covering the external vaginal opening. Its elasticity and condition can vary depending on factors like sexual intercourse, disease, injury, or exercise. An imperforate hymen is a congenital condition where the hymen completely obstructs the vagina without an opening. It occurs in around 1 in 1000 births and is usually diagnosed when menstrual blood accumulates in adolescent girls. Surgical incision of the hymen is required to treat an imperforate hymen and relieve symptoms like pelvic pain and menstrual retention. Complications can include infections if not treated.











































































































