Download to read offline
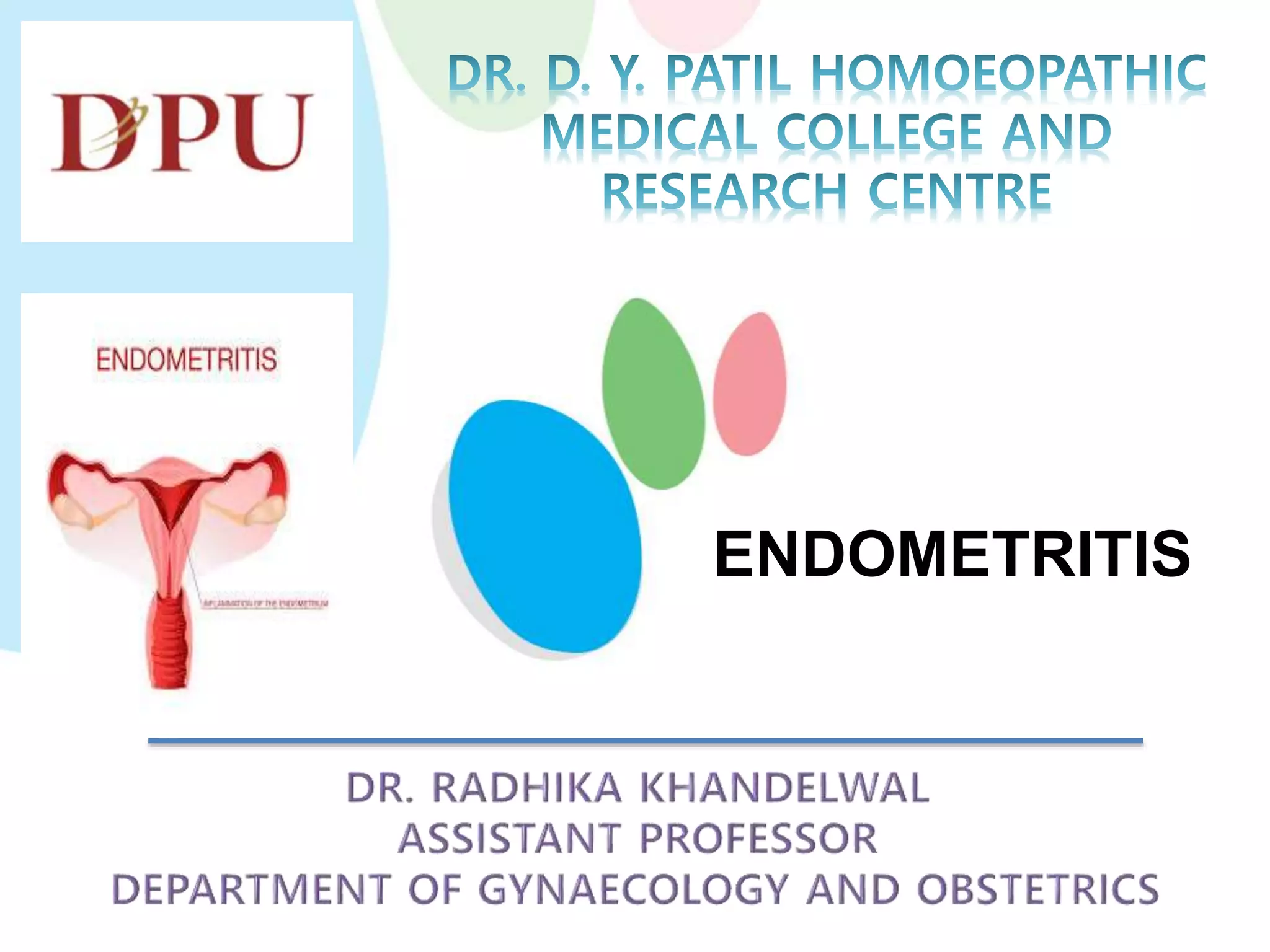


This document discusses endometritis, including acute, chronic, and atrophic types. Acute endometritis usually occurs after abortion or childbirth and is caused by various bacteria. Chronic endometritis results from a persistent infection in the uterine cavity caused by things like IUDs or retained products. Atrophic endometritis occurs in postmenopausal women due to loss of estrogen protection. Clinical features include vaginal discharge and abdominal or pelvic pain. Diagnosis involves tests like cervical smears, ultrasounds, and endometrial biopsies. Treatment involves removing the infection source and using antibiotics.











































































