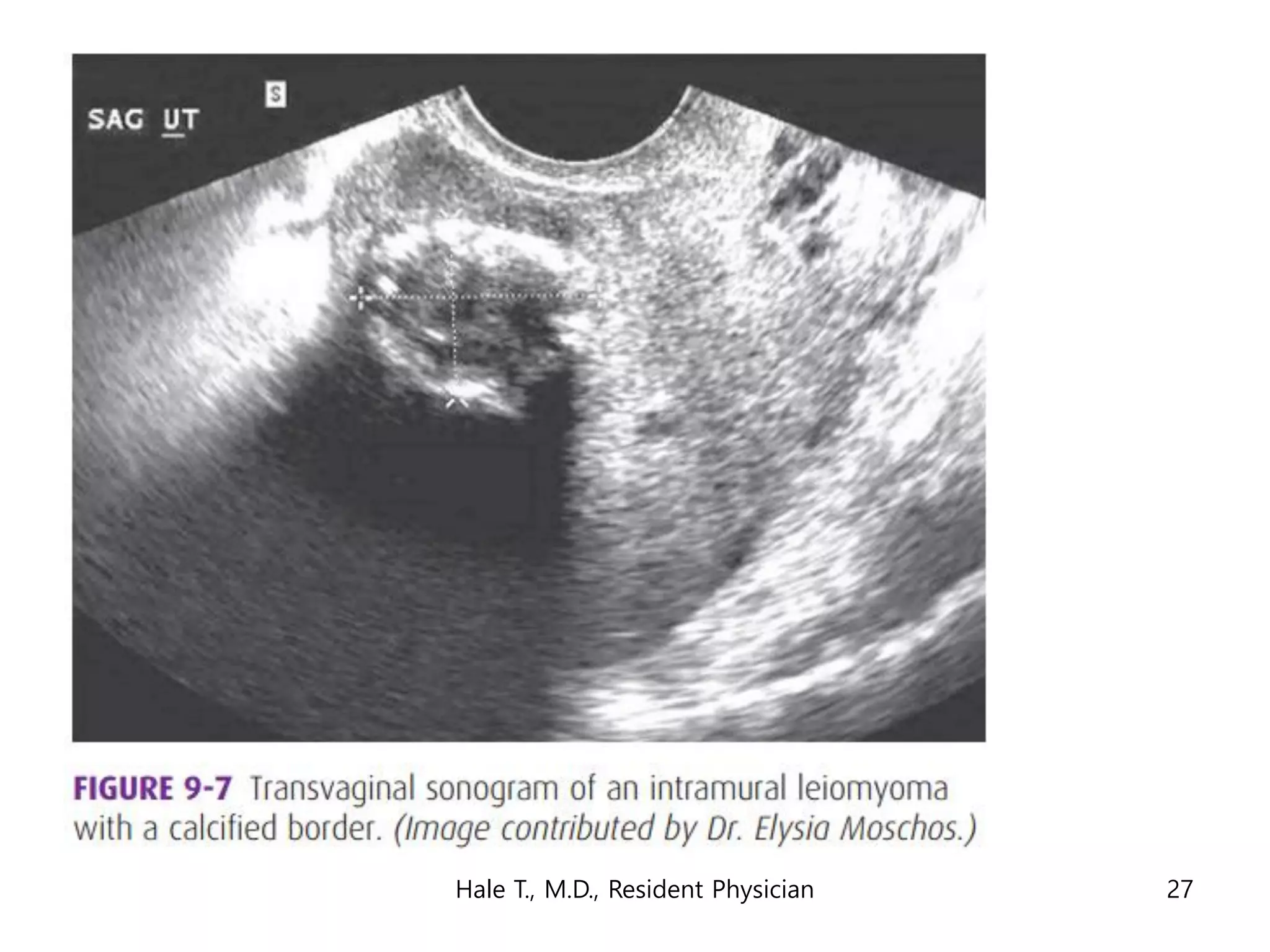
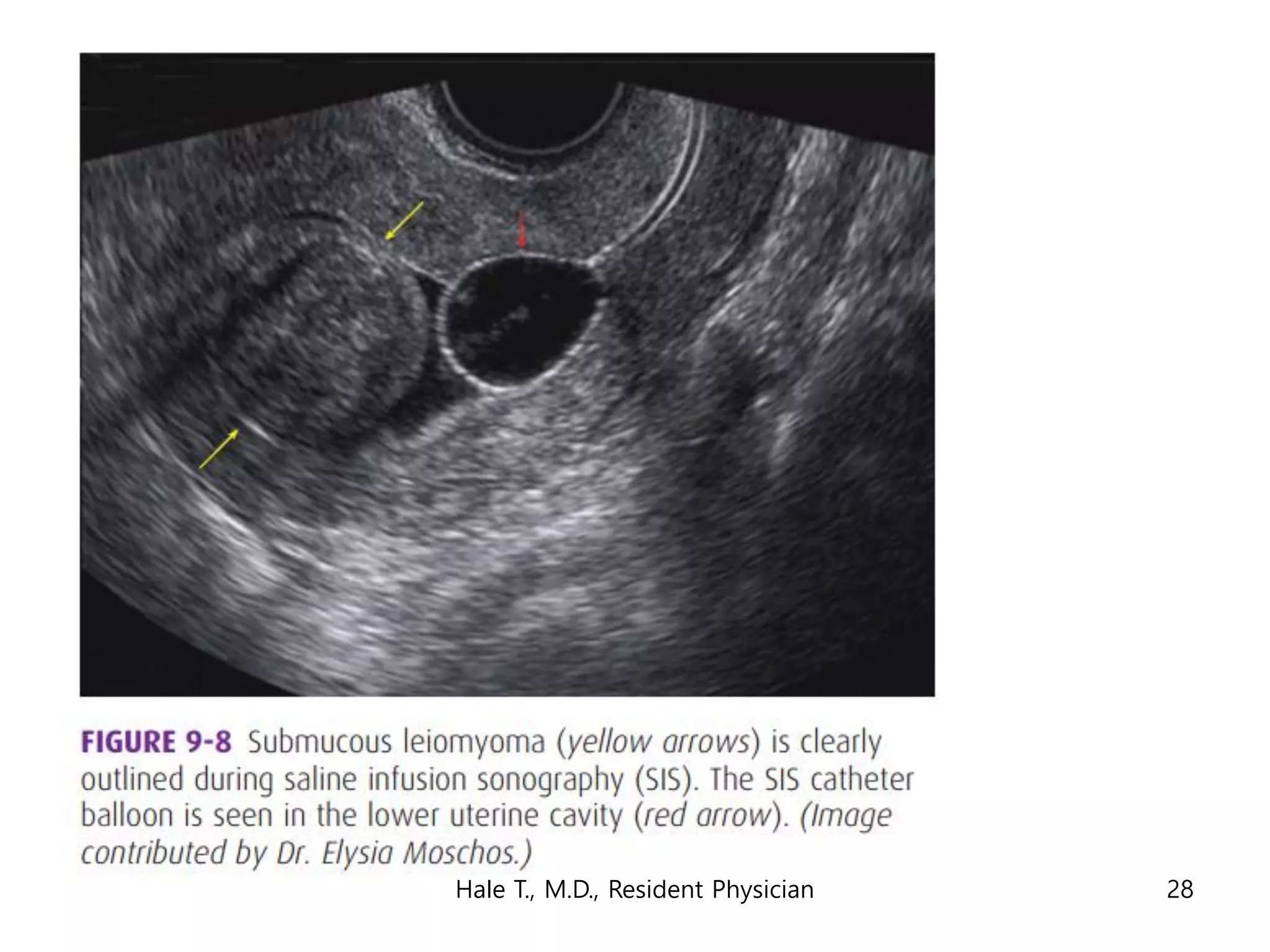
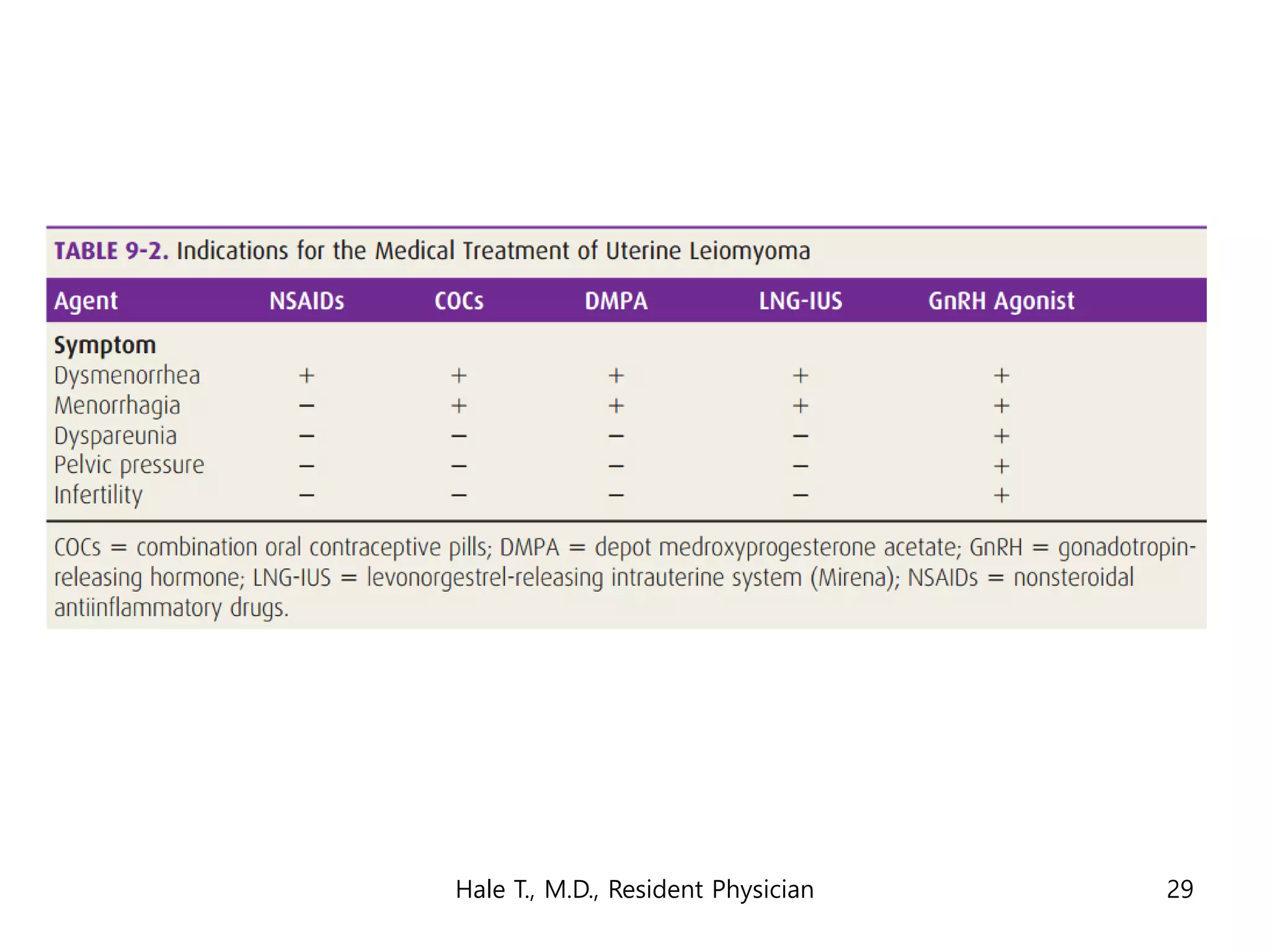
This document discusses myomas (uterine fibroids). It notes that myomas are benign smooth muscle tumors that originate in the uterus and are sensitive to estrogen and progesterone. Symptoms can include bleeding, pain, pressure, and infertility. Diagnosis is usually made through imaging like ultrasound or MRI. Treatment options include observation, drug therapy, uterine artery embolization, or surgical removal of the fibroids. The document also discusses complications that can arise if fibroids are present during pregnancy, such as pain, bleeding, preterm birth, and pregnancy loss.












































































![20. early pregnancy loss and ectopic pregnancy [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/20-180828222613-thumbnail.jpg?width=640&height=640&fit=bounds)






































