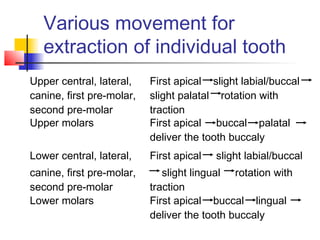
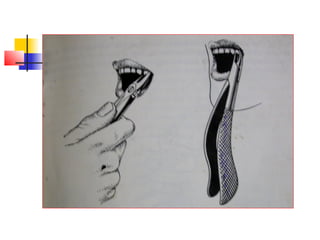
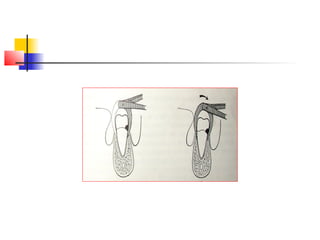
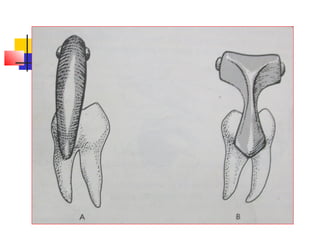
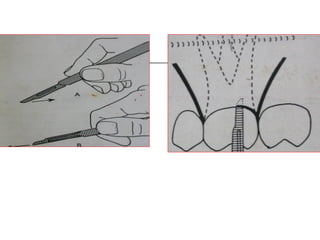
This document discusses different techniques for tooth extraction: forceps technique, elevator technique, and open/surgical extraction. It provides details on indications, contraindications, principles, and procedures for each technique. The forceps technique is preferred for mobile teeth and involves rotating and extracting the tooth. Elevators are used for impacted, malformed, or destroyed teeth by leveraging them out. Open extraction requires incisions and bone removal for grossly destroyed teeth or those near vital structures. Precise incisions and gentle tissue handling are emphasized for all extraction methods.