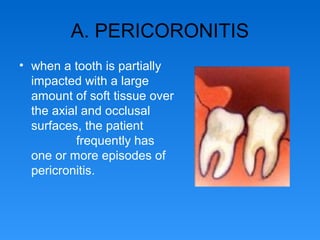
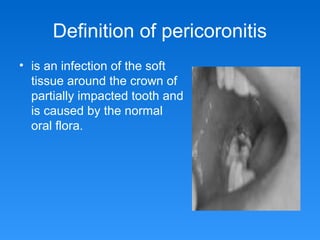
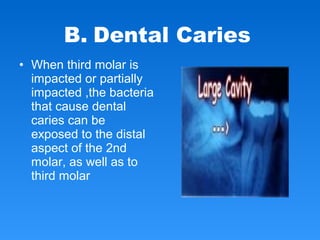
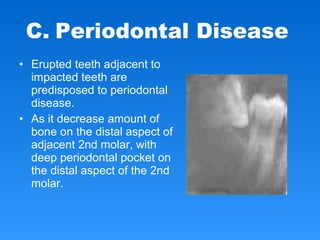
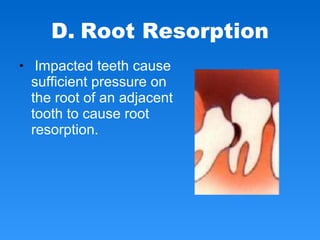
This document discusses dental impaction and surgical removal of impacted teeth. It defines impaction as a tooth failing to erupt into its normal position. Common causes include genetic syndromes, endocrine disorders, tumors, and arch length deficiencies. Mandibular third molars are most frequently impacted. Complications from impacted teeth include pericoronitis, caries, periodontal disease, root resorption, cysts, tumors, and fractures. Classification systems describe the position, depth, and angulation of impacted teeth to aid surgical planning. Surgical removal involves raising a flap, removing bone, delivering the tooth sometimes after division, preparing the site, and closing the wound. Postoperative care includes pressure, cold packs, and instructions