Downloaded 70 times











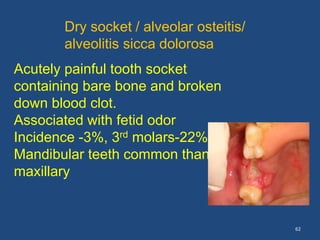
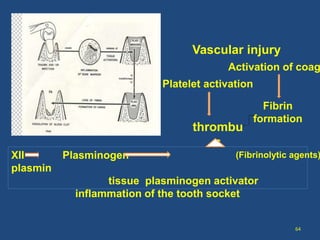
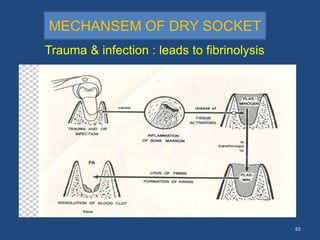




1. The document discusses complications that can arise from tooth extraction procedures. It classifies complications as immediate or delayed, and outlines various operative and postoperative complications including hemorrhage, nerve injury, bone fractures, and dry socket. 2. Risk factors for complications include patient medical conditions, surgical complexity, local anatomy, and clinician experience. Proper technique, anesthesia, and treatment can prevent or address many complications. 3. Dry socket is a painful condition where the tooth socket contains bare bone and broken blood clot. It may be caused by infection, trauma during extraction, use of vasoconstrictors, or patient factors like smoking.











































![Complications and management_slide[1] final to be put on slideshare](https://cdn.slidesharecdn.com/ss_thumbnails/complicationsandmanagementslide1finaltobeputonslideshare-130710114420-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
















