Downloaded 37 times

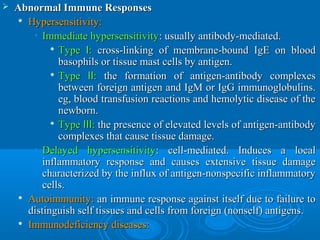
![ In the acute inflammation, localIn the acute inflammation, local
vasodilation increases blood flow in thevasodilation increases blood flow in the
inflamed tissue, and plasma proteins leakinflamed tissue, and plasma proteins leak
into the tissue due to increased vascularinto the tissue due to increased vascular
permeability.permeability.
Granulocytes monocyte / macrophages areGranulocytes monocyte / macrophages are
important cells in the non-specific responsesimportant cells in the non-specific responses
in innate immunity against pathogens.in innate immunity against pathogens.
Lymphocyte-driven responses andLymphocyte-driven responses and
antibodies have a significant role in theantibodies have a significant role in the
specific adaptive immunity and in chronicspecific adaptive immunity and in chronic
inflammation [1,2].inflammation [1,2].](https://image.slidesharecdn.com/immuno-pharmacology-160209071456/85/Immuno-pharmacology-2-320.jpg)
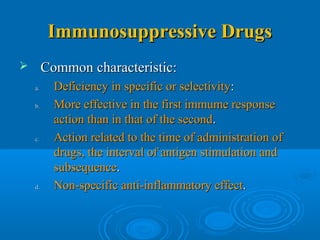
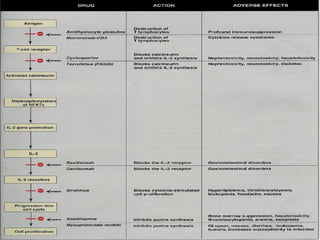
![ There are several anti-inflammatory and antirheumaticThere are several anti-inflammatory and antirheumatic
drugs which target lymphocyte receptors or pathwaysdrugs which target lymphocyte receptors or pathways
and suppress aberrant lymphocyte activation. Also,and suppress aberrant lymphocyte activation. Also,
inflammatory cytokines and other inflammatoryinflammatory cytokines and other inflammatory
mediators have been successful antiinflammatorymediators have been successful antiinflammatory
targets, and there are several novel cytokine-targetedtargets, and there are several novel cytokine-targeted
therapies under development for rheumatoid arthritistherapies under development for rheumatoid arthritis
[3] and other inflammatory diseases.[3] and other inflammatory diseases.
An interesting novel approach in the treatment ofAn interesting novel approach in the treatment of
arthritis is to target anti citrullinated protein antibodiesarthritis is to target anti citrullinated protein antibodies
(ACPAs) which are also known as biomarkers(ACPAs) which are also known as biomarkers
associated with worse prognosis and more erosiveassociated with worse prognosis and more erosive
disease [4, 5].disease [4, 5].](https://image.slidesharecdn.com/immuno-pharmacology-160209071456/85/Immuno-pharmacology-3-320.jpg)
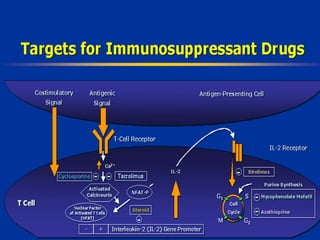
![ Eosinophilic granulocytes are important cells in theEosinophilic granulocytes are important cells in the
pathogenesis of asthma and other allergic disorderspathogenesis of asthma and other allergic disorders
[6,7]. In patients with asthma, eosinophils accumulate[6,7]. In patients with asthma, eosinophils accumulate
into the bronchial mucosa and release factors whichinto the bronchial mucosa and release factors which
maintain and exacerbate the inflammatory response,maintain and exacerbate the inflammatory response,
cause tissue injury and augment bronchoconstriction.cause tissue injury and augment bronchoconstriction.
Also, the lifespan and survival of eosinophils isAlso, the lifespan and survival of eosinophils is
prolonged in allergic states. Interestingly,prolonged in allergic states. Interestingly,
glucocorticoids induce apoptotic pathways inglucocorticoids induce apoptotic pathways in
eosinophils [8,9] resulting in accelerated clearance ofeosinophils [8,9] resulting in accelerated clearance of
eosinophils from the asthmatic lung.eosinophils from the asthmatic lung.
Therefore, induction of eosinophil apoptosis as aTherefore, induction of eosinophil apoptosis as a
therapeutic target in allergic asthma has attractedtherapeutic target in allergic asthma has attracted
increased attention [10].increased attention [10].](https://image.slidesharecdn.com/immuno-pharmacology-160209071456/85/Immuno-pharmacology-4-320.jpg)
![ Platelets play a central role in hemostasis. InPlatelets play a central role in hemostasis. In
addition, they are involved also in inflammationaddition, they are involved also in inflammation
and cancer through their interaction with otherand cancer through their interaction with other
cell types including leucocytes and endothelialcell types including leucocytes and endothelial
cells.cells.
Platelets are a rich source of various mediatorsPlatelets are a rich source of various mediators
including thromboxane A2 and other lipids, asincluding thromboxane A2 and other lipids, as
well as a wide number of angiogenic and growthwell as a wide number of angiogenic and growth
factors, and other proteins. The involvement offactors, and other proteins. The involvement of
platelets in inflammation and cancer, theplatelets in inflammation and cancer, the
detailed mechanisms and therapeutic strategiesdetailed mechanisms and therapeutic strategies
[11].[11].](https://image.slidesharecdn.com/immuno-pharmacology-160209071456/85/Immuno-pharmacology-5-320.jpg)
![ Disturbed interaction between the nervous andDisturbed interaction between the nervous and
immune systems has been implicated inimmune systems has been implicated in
various inflammatory diseases. The immunevarious inflammatory diseases. The immune
system can be considered as a ‘sixth sense’system can be considered as a ‘sixth sense’
which detects foreign agents such aswhich detects foreign agents such as
pathogens, allergens and tumour cells andpathogens, allergens and tumour cells and
interacts with the peripheral and centralinteracts with the peripheral and central
nervous system in many ways [12], & discussnervous system in many ways [12], & discuss
the role of the neuroimmune axis in thethe role of the neuroimmune axis in the
pathogenesis and future treatments of mentalpathogenesis and future treatments of mental
disorders [13].disorders [13].](https://image.slidesharecdn.com/immuno-pharmacology-160209071456/85/Immuno-pharmacology-6-320.jpg)

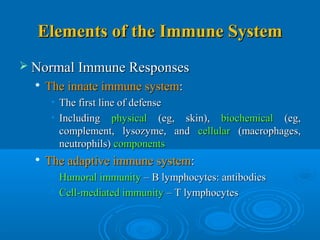


The document discusses the immune system and inflammation. It describes how the immune system protects the host from foreign molecules but can also result in problems like inflammation. Inflammation is characterized by redness, heat, swelling, pain and loss of function. These signs are caused by changes in blood vessels and cells driven by cytokines and other inflammatory mediators released during inflammation. The document also examines the role of various immune cells, cytokines and other mediators in both innate and adaptive immunity as well as the pathogenesis of diseases like arthritis, asthma and cancer. It explores potential therapeutic approaches targeting these mechanisms.


























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
