
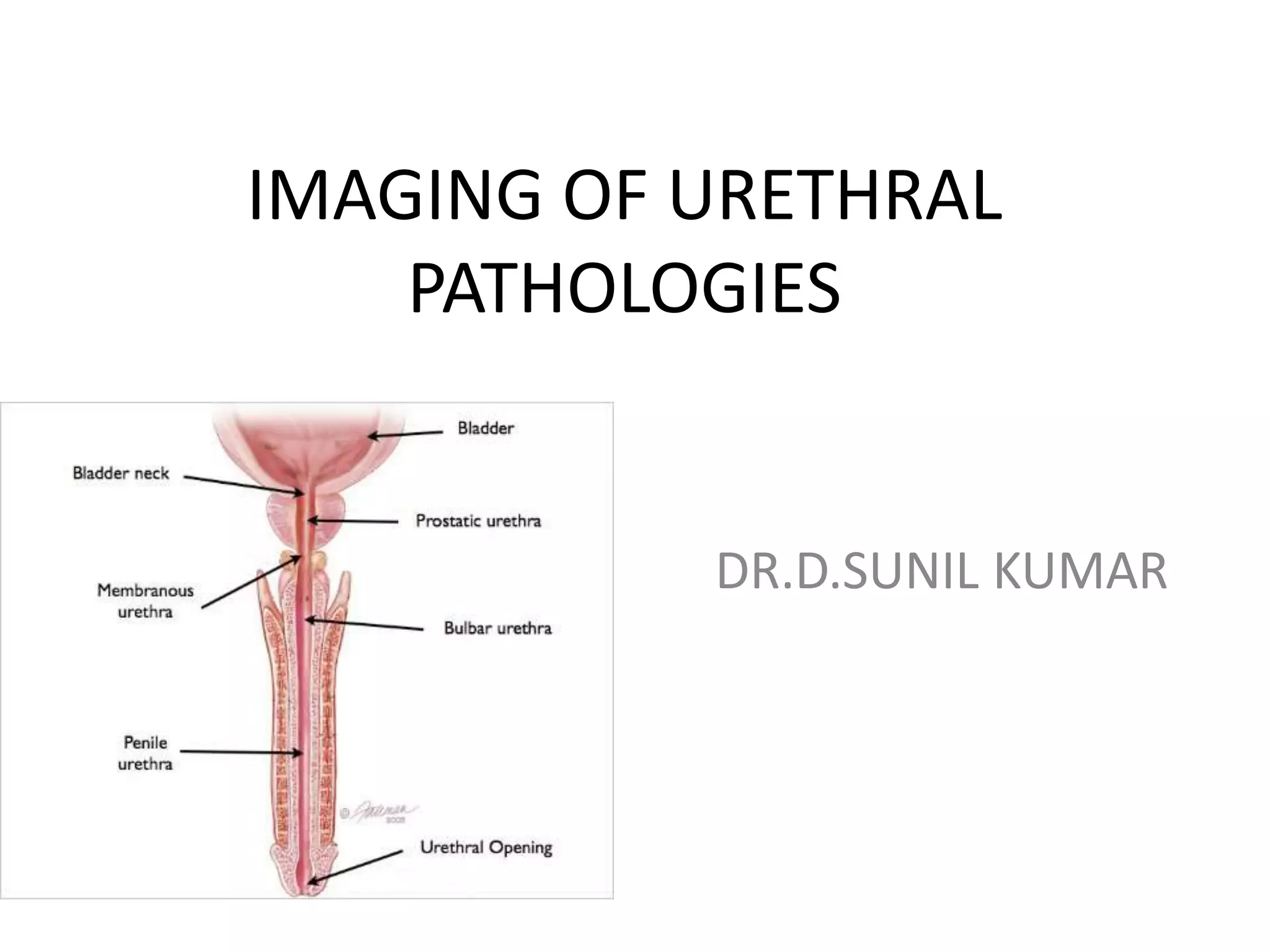
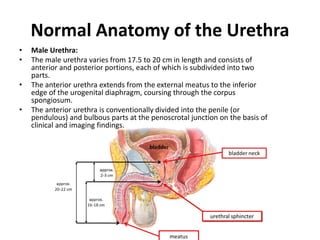
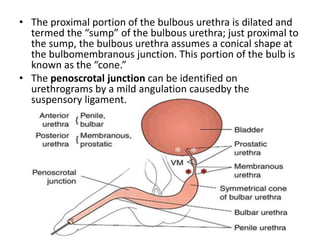
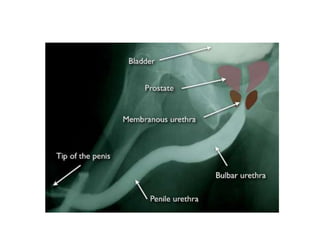
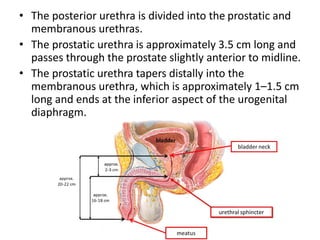
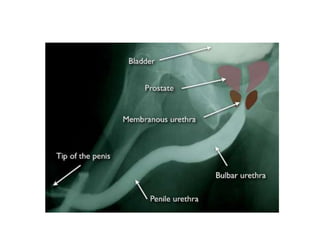
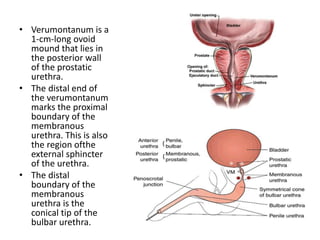

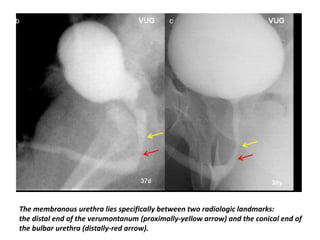
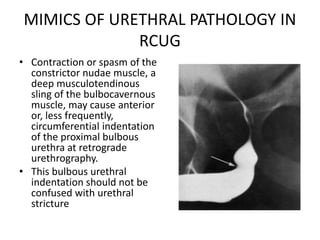
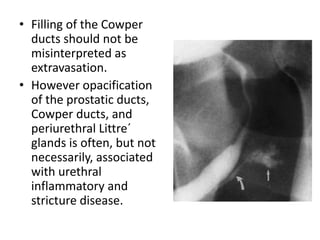


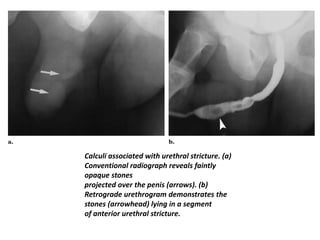

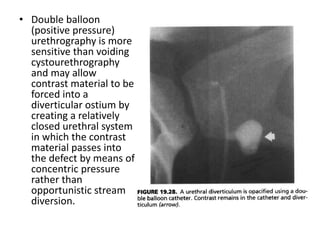


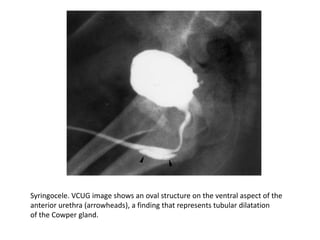


This document discusses the normal anatomy of the male and female urethra and various pathologies that can affect the urethra, as seen on medical imaging. For the male urethra, it describes the anatomy in detail and covers acquired inflammatory diseases like gonorrhea and nonspecific urethritis. It also discusses strictures, calculi, condyloma, and other conditions. For the female urethra, it briefly outlines the anatomy and mentions acquired urethral diverticula. Various imaging techniques for evaluating the urethra are also reviewed, including retrograde urethrography, ultrasonography, and others.





























































































