Downloaded 1,953 times































![References: Celiac Disease: Diagnostic clues to Unmaskan Imposter Malnick, Stephen, MD. Postgraduate Medicine 1997; 101: 239-244 Presutti J,Cangemi J, Cassidy H, Hill D, Celiac Disease. American Family Physician. December 15, 2007: 1795-1802 Lancet. 2003 Aug 2;362(9381):383-91.Celiac disease. Green PH, Jabri B. Department of Medicine, Columbia University College of Physicians and Surgeons, New York 10032, USA [email_address] Celiac Disease: Diagnostic clues to Unmaskan Imposter Malnick, Stephen, MD. Postgraduate Medicine 1997; 101: 239-244 Krause's book 2008. 681-684 (1352)-Disease of the small intestine-celiac disease](https://image.slidesharecdn.com/myprojectfinallanimationfinaaalr-111220112434-phpapp01/75/celiac-disease-34-2048.jpg)




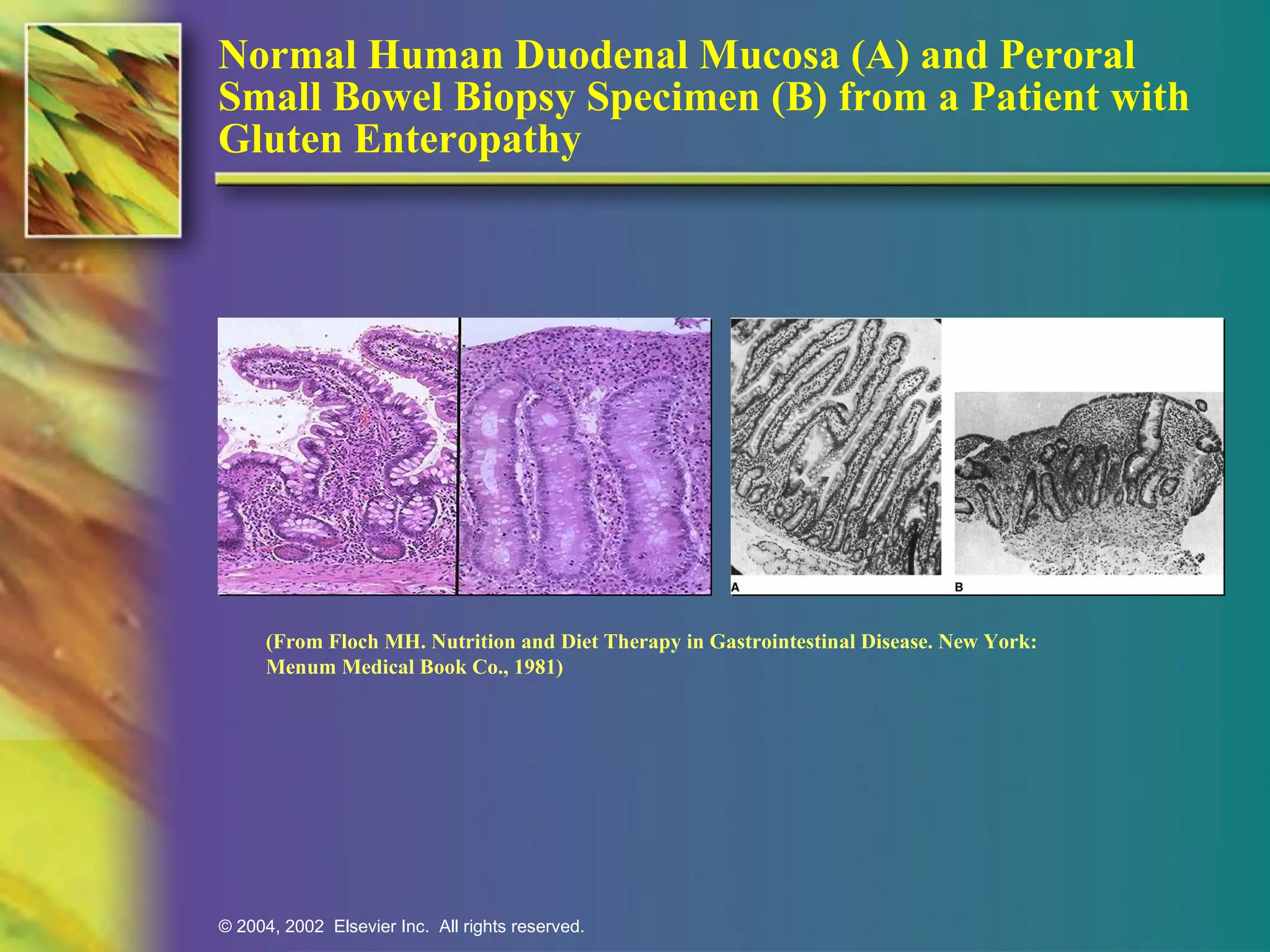
Celiac disease is an inherited autoimmune disorder where individuals cannot tolerate gluten from wheat, rye, and barley, leading to damage in the small intestine and poor nutrient absorption. The primary treatment is strict adherence to a gluten-free diet, which can improve overall health and requires lifelong commitment. Diagnosis involves blood tests and usually a biopsy of the small intestine to confirm the condition.



































































