Care pathway tomanage
depressive symptoms
Professor: Doha Rasheedy
Geriatrics and Gerontology department, Faculty of Medicine
Ain Shams University
Doha Rasheedy
2.
Agenda
• The riskfactors, and clinical presentation of
depression in the elderly.
• The comprehensive evaluation process for depressive
symptoms in older adults
• The importance of a holistic approach in managing
depression in elderly patients.
• The follow-up plan and support to enhance adherence
to treatment and improve outcomes.
• Final tips & takeaways
Doha Rasheedy
Case 1
• Mrs.S, an 82-year-old retired teacher, was brought to the clinic by her
daughter due to concerns about her increasing forgetfulness and
refusing to participate in outdoor activities.
• Mrs. S occasionally misplaces items and struggles to find words but can
still manage her daily activities independently. She has become less
interested in her favorite activities, including gardening and knitting. She
often declines invitations to family gatherings.
• She complains of mild fatigue and occasional headaches but denies any
significant pain. Her sleep is disturbed, with early morning awakenings.
Her appetite is mildly reduced, leading to a 2 kg weight loss over three
months.
• Mrs. S lost her husband one year ago.
• Cognitive Testing: she appeared not intreseted in performing the test yet
she reported normal orientation to time and place. Mild difficulty with
attention and short-term recall.
• Physical Exam: Normal, with no neurological deficits.
5.
Questions
• What arethe possible differential dianosis?
• How would you proceed next?
6.
• The differentialdiagnosis included early cognitive impairment, hypothyroidism,
anemia, grief and depression.
Next steps:
• Indepth history: other physical complaints, other mood related symptoms” low
mood, anhedonia, guilt, suicidality), the adaptation level after spouse loss.,
medication history should be reviewed
• Examination: Look for pallor (anemia), signs of hypothyroidism (bradycardia, dry
skin), or other systemic clues. Look for clues of neglect of personal care and
hygiene, refusal to engage in the interview.
• Perform GDS and may need to repeat cognitive screening if still affected perform
brain imaging.
• CBC, TSH
• Encourage physical activity
• Sleep hygiene
7.
• Depression remainsconsistently underdiagnosed and undertreated,
primarily due to factors such as underreporting driven by perceived stigma
and the widespread misconception that depression is a natural
consequence of aging.
• Additionally, depression in this population often presents as somatic
symptoms, which are frequently misinterpreted as indications of underlying
medical conditions
• Mrs. S.,an 82-year-old widow, presented to a geriatric clinic with
complaints of persistent low mood, fatigue, and lack of interest in her
usual activities for the past six months. She had difficulty sleeping,
poor appetite, and expressed feelings of worthlessness. Her medical
history included hypertension, type 2 diabetes, fibromyalgia, urinary
incontinence, mild cognitive impairment, and visual impairment. Mrs.
S. lived alone, with limited social interactions, and faced financial
hardships that added to her stress.
• What are the risk factors for Mrs. feeling of worthlessness?
• Apply DSM 5 criteria for depression in this case?
• What are other risk factors increases depression in older adults?
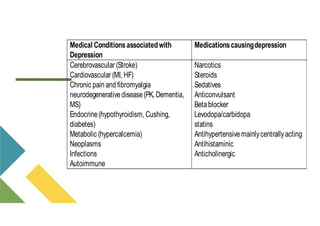
• Are there any medical conditions and/or mediactions that could increase the risk of
depressed mood in older adults?
10.
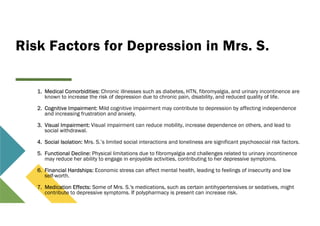
Risk Factors forDepression in Mrs. S.
1. Medical Comorbidities: Chronic illnesses such as diabetes, HTN, fibromyalgia, and urinary incontinence are
known to increase the risk of depression due to chronic pain, disability, and reduced quality of life.
2. Cognitive Impairment: Mild cognitive impairment may contribute to depression by affecting independence
and increasing frustration and anxiety.
3. Visual Impairment: Visual impairment can reduce mobility, increase dependence on others, and lead to
social withdrawal.
4. Social Isolation: Mrs. S.’s limited social interactions and loneliness are significant psychosocial risk factors.
5. Functional Decline: Physical limitations due to fibromyalgia and challenges related to urinary incontinence
may reduce her ability to engage in enjoyable activities, contributing to her depressive symptoms.
6. Financial Hardships: Economic stress can affect mental health, leading to feelings of insecurity and low
self-worth.
7. Medication Effects: Some of Mrs. S.'s medications, such as certain antihypertensives or sedatives, might
contribute to depressive symptoms. If polypharmacy is present can increase risk.
11.
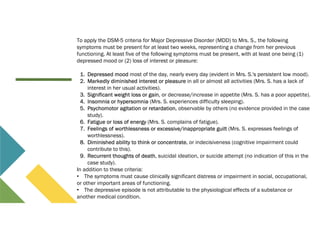
To apply theDSM-5 criteria for Major Depressive Disorder (MDD) to Mrs. S., the following
symptoms must be present for at least two weeks, representing a change from her previous
functioning. At least five of the following symptoms must be present, with at least one being (1)
depressed mood or (2) loss of interest or pleasure:
1. Depressed mood most of the day, nearly every day (evident in Mrs. S.'s persistent low mood).
2. Markedly diminished interest or pleasure in all or almost all activities (Mrs. S. has a lack of
interest in her usual activities).
3. Significant weight loss or gain, or decrease/increase in appetite (Mrs. S. has a poor appetite).
4. Insomnia or hypersomnia (Mrs. S. experiences difficulty sleeping).
5. Psychomotor agitation or retardation, observable by others (no evidence provided in the case
study).
6. Fatigue or loss of energy (Mrs. S. complains of fatigue).
7. Feelings of worthlessness or excessive/inappropriate guilt (Mrs. S. expresses feelings of
worthlessness).
8. Diminished ability to think or concentrate, or indecisiveness (cognitive impairment could
contribute to this).
9. Recurrent thoughts of death, suicidal ideation, or suicide attempt (no indication of this in the
case study).
In addition to these criteria:
• The symptoms must cause clinically significant distress or impairment in social, occupational,
or other important areas of functioning.
• The depressive episode is not attributable to the physiological effects of a substance or
another medical condition.
12.
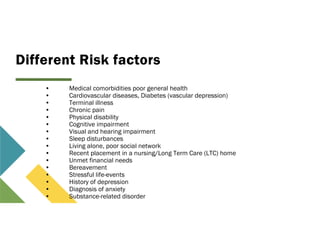
Different Risk factors
•Medical comorbidities poor general health
• Cardiovascular diseases, Diabetes (vascular depression)
• Terminal illness
• Chronic pain
• Physical disability
• Cognitive impairment
• Visual and hearing impairment
• Sleep disturbances
• Living alone, poor social network
• Recent placement in a nursing/Long Term Care (LTC) home
• Unmet financial needs
• Bereavement
• Stressful life-events
• History of depression
• Diagnosis of anxiety
• Substance-related disorder
Name: Mr. AhmedElSayed
Age: 78 years
Gender: Male
Medical History: Hypertension, Type 2 Diabetes Mellitus (DM), Coronary Artery Disease,
Hyperlipidemia, Osteoarthritis
• Mr. Ahmed presented to the emergency department with sudden onset right sided hemiplegia, facial drooping, and slurred speech.
A brain CT scan confirmed an acute ischemic stroke in the left middle cerebral artery territory.
• Thrombolytic therapy was not indicated due to late presentation. He was managed with antiplatelet therapy, statins, and blood
pressure control.
• Antihypertensives, oral hypoglycemics, and lipidlowering agents were optimized.
Mr. Ahmed was enrolled in a multidisciplinary rehabilitation program, including:
• Physical Therapy: To improve motor function and mobility.
• Occupational Therapy: To enhance activities of daily living (ADLs).
• Speech Therapy: For mild dysarthria.
• Mr. Ahmed was enrolled in a multidisciplinary rehabilitation program, including:
• Physical Therapy: To improve motor function and mobility.
• Occupational Therapy: To enhance activities of daily living (ADLs).
• Speech Therapy: For mild dysarthria.
16.
• In thesecond month, Mr. Ahmed became withdrawn, showed a lack of interest
in therapy sessions, and had poor sleep and appetite. His family reported
irritability and feelings of hopelessness.
• In the second month, Mr. Ahmed became withdrawn, showed a lack of interest
in therapy sessions, and had poor sleep and appetite. His family reported
irritability and feelings of hopelessness.
• His blood pressure became uncontrolled (160/100 mmHg), and his HbA1c
increased to 9%. His physical improvement plateaued, and he became more
dependent in his ADLs.
• What is the cause for the deterioration in Mr Ahmed’s case?
• What is the suggested approach for this case?
• What are the investigations recpmmended for elders with first episode non
perciptated depressive symptoms?
17.
Post stroke depressionis the cause for
the deterioration observed
1. Screening for depressive disorders using validated tools
Positive screening outcomes necessitate a comprehensive follow-up evaluation to assess the severity of
depression, identify coexisting psychological disorders, consider alternative diagnoses, and account for any
underlying medical conditions.
1. comprehenasive evaluation:
1. Analyse depressive symptoms including suicidal risk and evaluate all physical symptoms.
2. Apply the diagnostic criteria DSM-5
3. Exclude underlying cognitive deficit or medical disorder responsible for the symptoms.
4. Assessment of functional capacity
5. Social assessment and caregiver evaluation
6. Physical examination and investigations
7. Refer to psychiatrist for a detailed psychiatric assessment
18.
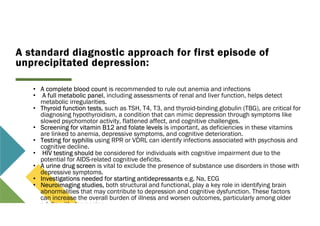
A standard diagnosticapproach for first episode of
unprecipitated depression:
• A complete blood count is recommended to rule out anemia and infections
• A full metabolic panel, including assessments of renal and liver function, helps detect
metabolic irregularities.
• Thyroid function tests, such as TSH, T4, T3, and thyroid-binding globulin (TBG), are critical for
diagnosing hypothyroidism, a condition that can mimic depression through symptoms like
slowed psychomotor activity, flattened affect, and cognitive challenges.
• Screening for vitamin B12 and folate levels is important, as deficiencies in these vitamins
are linked to anemia, depressive symptoms, and cognitive deterioration.
• Testing for syphilis using RPR or VDRL can identify infections associated with psychosis and
cognitive decline.
• HIV testing should be considered for individuals with cognitive impairment due to the
potential for AIDS-related cognitive deficits.
• A urine drug screen is vital to exclude the presence of substance use disorders in those with
depressive symptoms.
• Investigations needed for starting antidepressants e.g. Na, ECG
• Neuroimaging studies, both structural and functional, play a key role in identifying brain
abnormalities that may contribute to depression and cognitive dysfunction. These factors
can increase the overall burden of illness and worsen outcomes, particularly among older
adults with depression.
19.
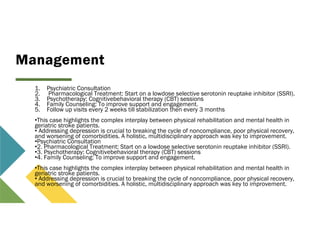
Management
1. Psychiatric Consultation
2.Pharmacological Treatment: Start on a lowdose selective serotonin reuptake inhibitor (SSRI).
3. Psychotherapy: Cognitivebehavioral therapy (CBT) sessions
4. Family Counseling: To improve support and engagement.
5. Follow up visits every 2 weeks till stabilization then every 3 months
•This case highlights the complex interplay between physical rehabilitation and mental health in
geriatric stroke patients.
• Addressing depression is crucial to breaking the cycle of noncompliance, poor physical recovery,
and worsening of comorbidities. A holistic, multidisciplinary approach was key to improvement.
•Psychiatric Consultation
•2. Pharmacological Treatment: Start on a lowdose selective serotonin reuptake inhibitor (SSRI).
•3. Psychotherapy: Cognitivebehavioral therapy (CBT) sessions
•4. Family Counseling: To improve support and engagement.
•This case highlights the complex interplay between physical rehabilitation and mental health in
geriatric stroke patients.
• Addressing depression is crucial to breaking the cycle of noncompliance, poor physical recovery,
and worsening of comorbidities. A holistic, multidisciplinary approach was key to improvement.
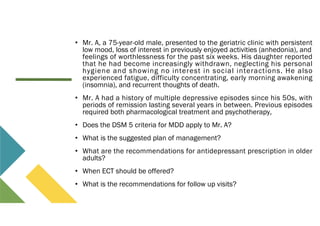
• Mr. A,a 75-year-old male, presented to the geriatric clinic with persistent
low mood, loss of interest in previously enjoyed activities (anhedonia), and
feelings of worthlessness for the past six weeks. His daughter reported
that he had become increasingly withdrawn, neglecting his personal
hygiene and showing no interest in social interactions. He also
experienced fatigue, difficulty concentrating, early morning awakening
(insomnia), and recurrent thoughts of death.
• Mr. A had a history of multiple depressive episodes since his 50s, with
periods of remission lasting several years in between. Previous episodes
required both pharmacological treatment and psychotherapy,
• Does the DSM 5 criteria for MDD apply to Mr. A?
• What is the suggested plan of management?
• What are the recommendations for antidepressant prescription in older
adults?
• When ECT should be offered?
• What is the recommendations for follow up visits?
22.
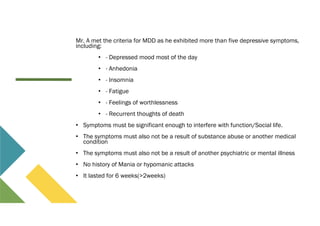
Mr. A metthe criteria for MDD as he exhibited more than five depressive symptoms,
including:
• - Depressed mood most of the day
• - Anhedonia
• - Insomnia
• - Fatigue
• - Feelings of worthlessness
• - Recurrent thoughts of death
• Symptoms must be significant enough to interfere with function/Social life.
• The symptoms must also not be a result of substance abuse or another medical
condition
• The symptoms must also not be a result of another psychiatric or mental illness
• No history of Mania or hypomanic attacks
• It lasted for 6 weeks(>2weeks)
23.
• a combinationof antidepressants (See next slide) and concurrent
psychotherapy.
• ECT should be considered if adequate trials of antidepressants combined
with psychotherapy have been ineffective or if the health of the patient is
deteriorating rapidly due to depression.
• Complementary therapy:
• Physical Activity
• Psychoeducation
• Supportive Care
• Nutritional Interventions
24.
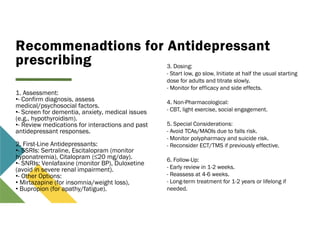
Recommenadtions for Antidepressant
prescribing
1.Assessment:
•- Confirm diagnosis, assess
medical/psychosocial factors.
•- Screen for dementia, anxiety, medical issues
(e.g., hypothyroidism).
•- Review medications for interactions and past
antidepressant responses.
2. First-Line Antidepressants:
•- SSRIs: Sertraline, Escitalopram (monitor
hyponatremia), Citalopram (≤20 mg/day).
•- SNRIs: Venlafaxine (monitor BP), Duloxetine
(avoid in severe renal impairment).
•- Other Options:
• Mirtazapine (for insomnia/weight loss),
• Bupropion (for apathy/fatigue).
3. Dosing:
- Start low, go slow. Initiate at half the usual starting
dose for adults and titrate slowly.
- Monitor for efficacy and side effects.
4. Non-Pharmacological:
- CBT, light exercise, social engagement.
5. Special Considerations:
- Avoid TCAs/MAOIs due to falls risk.
- Monitor polypharmacy and suicide risk.
- Reconsider ECT/TMS if previously effective.
6. Follow-Up:
- Early review in 1-2 weeks.
- Reassess at 4-6 weeks.
- Long-term treatment for 1-2 years or lifelong if
needed.
25.
Indications for ECT
•suicidal or homicidal risk or present in a catatonic, psychotic, agitated, or
medically unstable state, symptoms are refractory to pharmacotherapy.
• Caution is adviced in applying ECT in the following conditions:
• Intracranial lesions: Risk of edema/brain herniation post-ECT.
• Cardiac risks: Unstable angina, CHF, uncontrolled HTN, high-grade AV block,
ventricular arrhythmias.
• Pulmonary risks: Severe COPD, asthma, pneumonia.
• Metabolic risks: Hypo-/hyperkalemia.
26.
The suggested plan
•Initiation of an SSRI (Selective Serotonin Reuptake Inhibitor),
considering age-appropriate dosing
• Engagement in cognitive-behavioral therapy (CBT)
• Regular follow-up to monitor response to treatment and assess
suicide risk
27.
Follow up plan
•Frequency of follow up visits: every 2 weeks till stabilization then every 3 months
• The follow up visit include:
• a) Assess compliance
• b) Assess response to treatment, decide dose titration or discontinuation
• c) Monitor drug side effects: A serum sodium level should be done within 2–4
weeks of initiating SSRI or SNRI antidepressants. Prescribers may consider checking
the level after 2 weeks for those patients on diuretics or who have a history of
hyponatremia. There is a lower of risk of hyponatremia with TCAs, bupropion, and
mirtazapine
• d) Assess suicide risk
• e) monitoring for worsening of depression, agitation, and suicide risk.
28.
Final tips &
takeaways
•Consider medical, psychological, and social factors contributing
to depressive symptoms. Use a comprehensive geriatric
assessment approach.
• Distinguish between depression, dementia, and delirium.
Remember that somatic complaints or cognitive impairment can
be symptoms of depression in older adults.
• Develop individualized treatment plans combining
pharmacological and non-pharmacological approaches,
including psychotherapy, social engagement, and physical
activity.
• Regularly evaluate treatment efficacy and adjust the plan as
needed. Be vigilant for signs of treatment non-adherence or
worsening symptoms.


























































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)











![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)
