Downloaded 24 times

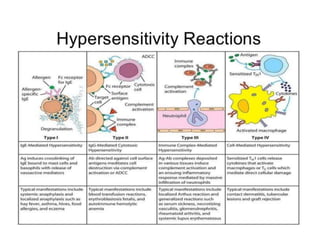
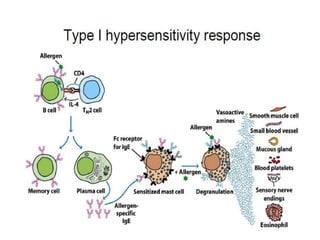

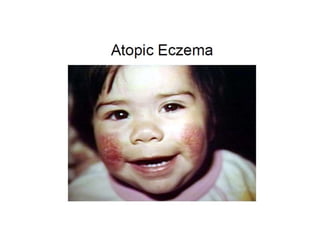
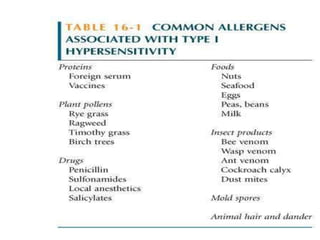
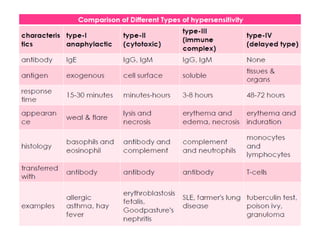


Hypersensitivity involves negative immune reactions, such as allergies, that can range from mild to life-threatening, and is classified into four types based on their mechanism and timing. Type I hypersensitivity is immediate and often involves reactions like anaphylaxis, while Types II and III involve cytotoxic responses and immune complex reactions respectively. Diagnostic and treatment approaches vary but may include skin tests, corticosteroids, and immunotherapy.
















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

