Downloaded 573 times
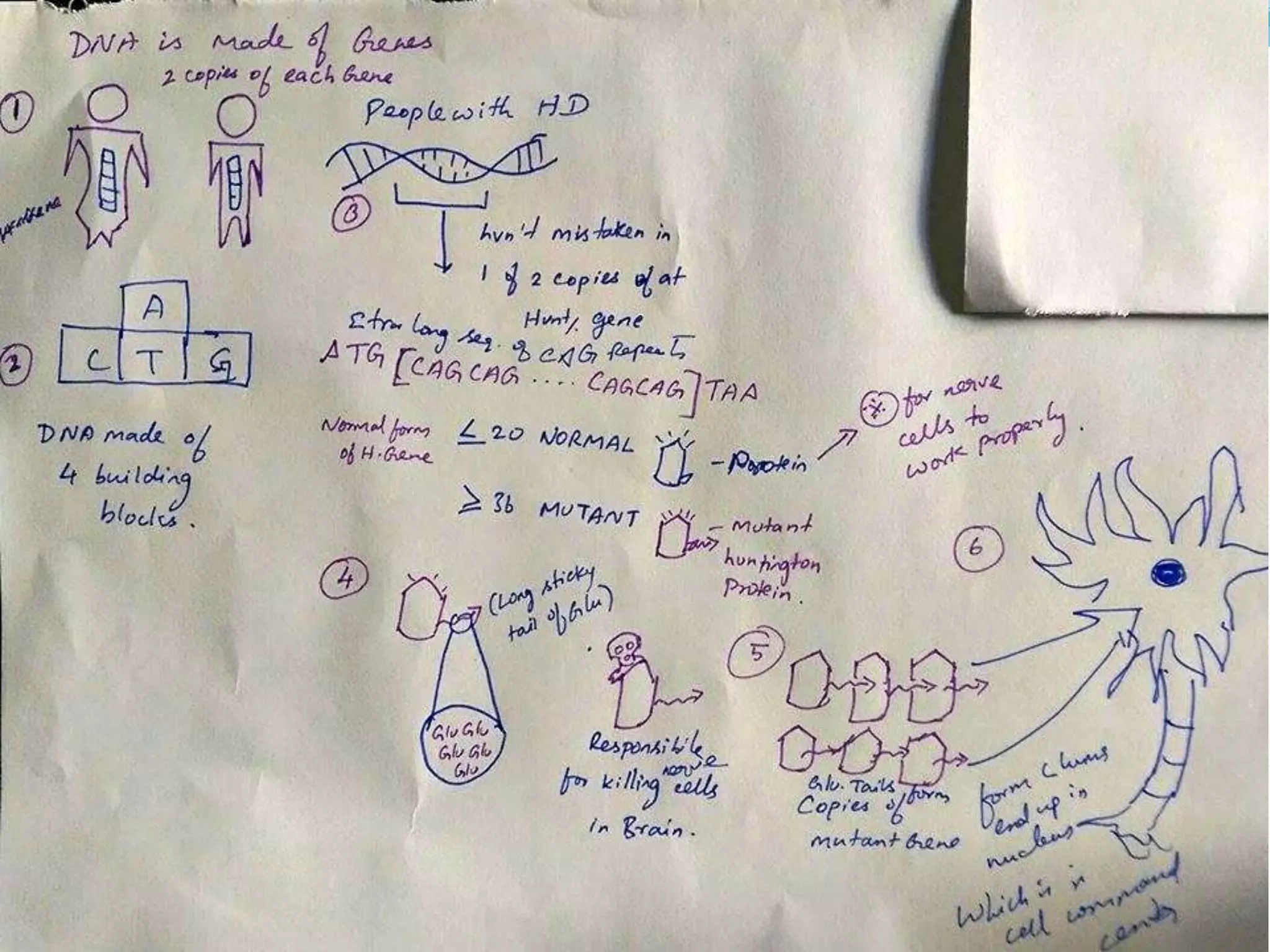



Huntington's disease is a neurodegenerative genetic disorder that causes the progressive breakdown of nerve cells in the brain, especially in the basal ganglia. It affects movement, cognition, and psychiatric functions and is caused by a defective gene inherited from a parent. Symptoms typically appear between ages 30-50 and include involuntary movements, cognitive decline, and psychiatric issues like depression. While there is no cure, treatment aims to reduce symptoms and complications through medications, speech/occupational/physical therapy, and supportive care.























































































