










![Patients have decreased lung volumes or TLC (total lung capacity) with normal airflow
(normal FEV1/FVC ratio but with reduced values for both FVC and FEV1 individually). There are
five primary types:
Pleural--diseases of the pleura that restrict lung expansion and decrease lung volumes (eg,
pleural effusions or pleural thickening).
Alveolar--diseases of alveolar spaces that prevent air from filling those same spaces (eg,
pneumonia, cancer, and pulmonary edema).
Interstitial--various diseases contracting the space in the lung parenchyma between the
alveoli (interstitium), reducing lung volumes (eg, sarcoidosis, pulmonary fibrosis, silicosis,
and pneumoconiosis).
Neuromuscular--Normal lung parenchyma with an inability to take a deep breath (eg,
diaphragmatic paralysis, Guillain-BarrŽ syndrome, myasthenia gravis, and amyotrophic lateral
sclerosis).
Thoracic cage--Skeletal abnormalities with normal lungs (eg, kyphoscoliosis, obesity).
Obstructive lung diseases Restrictive lung diseases
Affect the patency or elasticity of the airways, Interfere in or change chest wall or lung
leading to an increase in airway resistance parenchyma
Expiration is primarily affected Inspiration is primarily affected
Vital capacity is decreased Vital capacity is normal or decreased
Total lung capacity is increased Total lung capacity is decreased
Residual volume is increased Residual volume is decreased
Indications and Contraindications of Oxygen Therapy
Indications
A change in the patient’s respiratory rate or pattern may be one of the earliest indicators
of the need for oxygen therapy. The change in respiratory rate or pattern may result from
hypoxemia or hypoxia. The signs and symptoms signaling the need for oxygen may depend on
how suddenly this need develops. With rapidly developing hypoxia, changes occur in the central
nervous system because the higher neurologic centers are very sensitive to oxygen deprivation.
The clinical picture may resemble that of alcohol intoxication, with the patient exhibiting lack of
coordination and impaired judgment. Longstanding hypoxia (as seen in chronic obstructive
pulmonary disease [COPD] and chronic heart failure) may produce fatigue, drowsiness, apathy,
inattentiveness, and delayed reaction time. The need for oxygen is assessed by arterial blood gas
analysis and pulse oximetry as well as by clinical evaluation.
Contraindications
Oxygen should never be used in explosive environments, and its use is cautioned against
when there is a risk of sparks or materials combusting as oxygen accelerates combustion.
Smoking during oxygen therapy is a fire hazard and a danger to life and limb, especially with
home oxygen if compliance is poor. Oxygen may worsen the effects of paraquat poisoning and is
therefore contraindicated in such cases. Oxygen therapy is not recommended for patients who
have suffered pulmonary fibrosis or other lung damage resulting from Bleomycin treatment.
OXYGEN TOXICITY
Oxygen toxicity may occur when too high a concentration of oxygen (greater than 50%) is
HS 194 | 1/7/2010
administered for an extended period (longer than 48 hours). It is caused by overproduction of
oxygen free radicals, which are byproducts of cell metabolism. If oxygen toxicity is untreated,
these radicals can severely damage or kill cells.
Antioxidants such as vitamin E, vitamin C, and beta-carotene may help defend against
oxygen free radicals (Scanlan, Wilkins & Stoller, 1999). The dietitian can adjust the patient’s diet
14](https://image.slidesharecdn.com/hs194-galicinaoreyneldan-101222175930-phpapp02/85/Hs-194-15-320.jpg)




























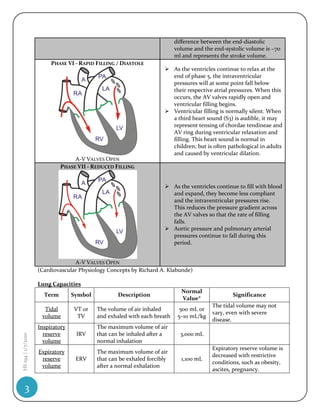
This document discusses the phases of the cardiac cycle: 1) There are seven phases of the cardiac cycle that describe the contraction and relaxation of the atria and ventricles as well as the opening and closing of valves. 2) The phases include atrial contraction, isovolumetric contraction, rapid ejection, reduced ejection, isovolumetric relaxation, rapid filling, and reduced filling. 3) Each phase is characterized by the state of the atrioventricular and semilunar valves as well as the electrical and mechanical events that occur in the atria and ventricles.










































































