Downloaded 544 times
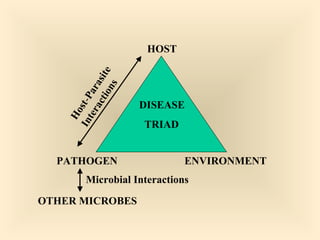
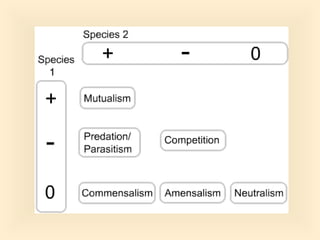







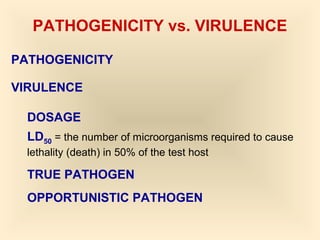


























The document discusses the interactions between pathogens, the environment, and hosts, detailing how infections occur through various portals of entry and factors that contribute to infectious disease. It outlines the types of pathogens, the concept of colonization, and differentiates between infection and disease, emphasizing virulence factors such as toxins and microbial resistance. Additionally, it covers the epidemiology of nosocomial infections and the body's immune responses to pathogens.










































































