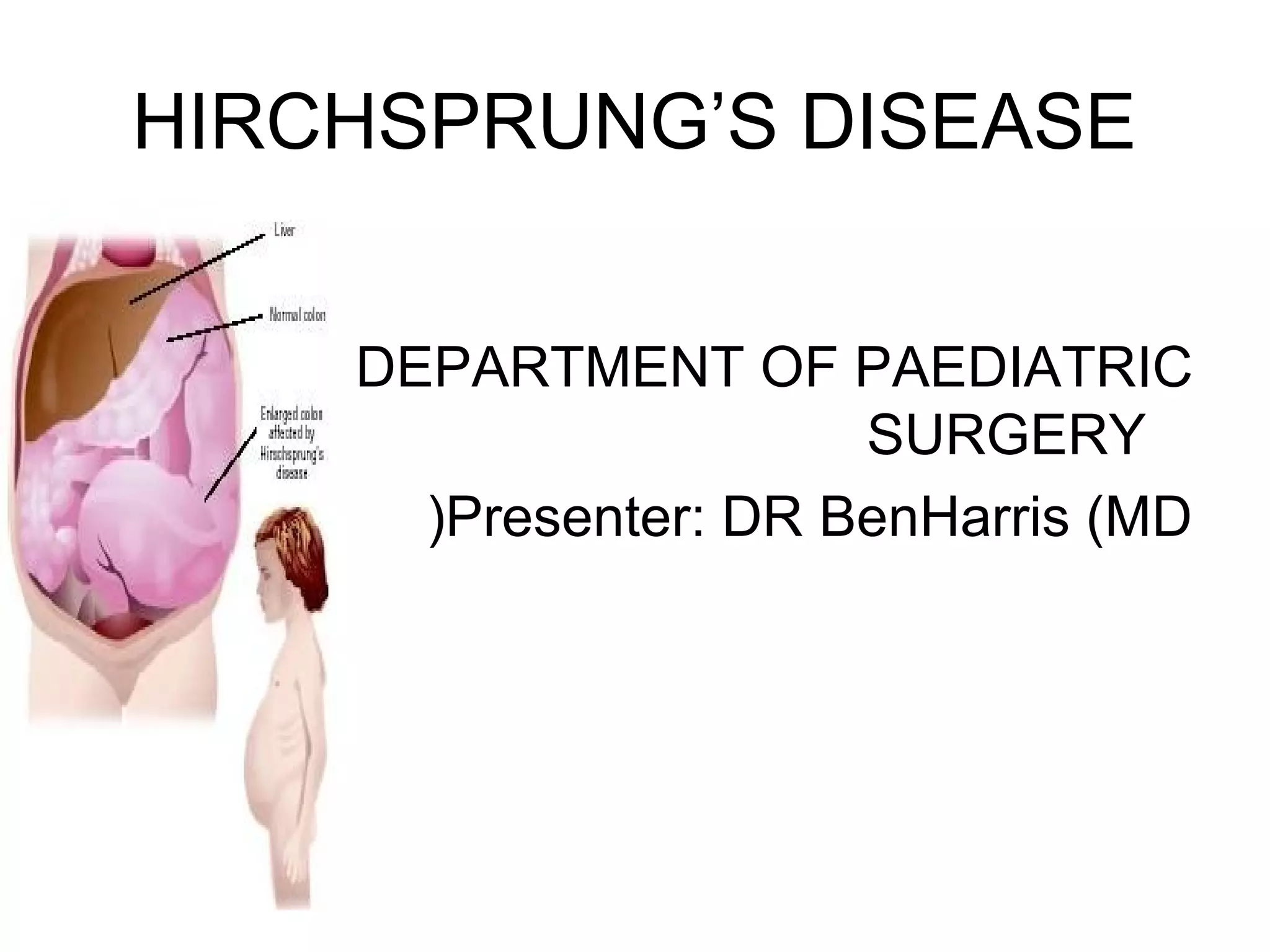
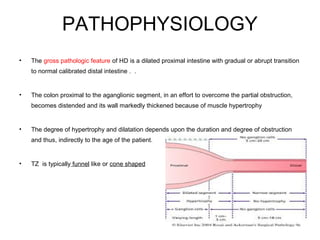
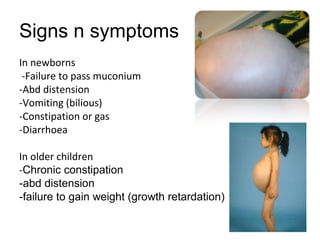
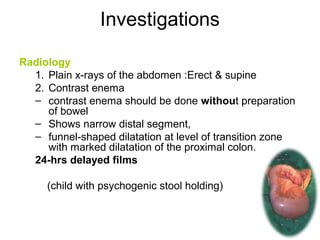
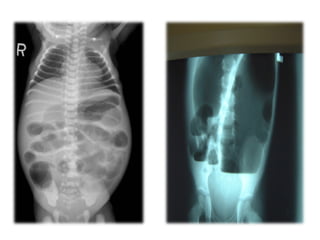
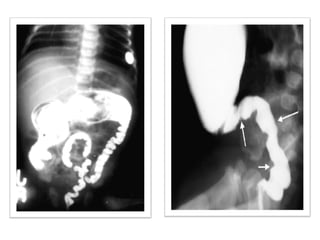
Hirschsprung's disease is a congenital condition caused by the lack of nerve cells in parts of the colon, preventing normal contraction. It is most commonly due to mutations in RET, EDNRB or EDN3 genes. Symptoms include constipation, abdominal distension and vomiting in newborns. Diagnosis involves biopsy and imaging showing dilated bowel above a narrowed transition zone. Treatment is initially with colostomy, then definitive surgery like pull-through procedures to remove the affected bowel segment. Complications can include infection and incontinence.