Hepatitis viruses - A,B & C
•Download as PPT, PDF•
7 likes•2,799 views

This talks about the HAV, HBV and HCV , intro, properties, epidemiology and transmission, pathogenesis , clinical findings , laboratory diagnosis, and prevention

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Hepatitis viruses - A,B & C
Similar to Hepatitis viruses - A,B & C (20)
More from Khaled AlKhodari
More from Khaled AlKhodari (20)
Recently uploaded
Recently uploaded (20)
Hepatitis viruses - A,B & C
- 1. HEPATITIS VIRUSES HAV-HBV-HCV BY : MOHAMMED ELBELBESSI (HAV) SADIY. NKAHALA (HBV) KHALED H.ALKHODARI (HCV) SUPERVISOR: DR. SAID S.ALGHORRA
- 2. Prepared by : Mohammed Elbelbessi Supervised by : Dr- Said El-ghora
- 3. 1- Introduction 2- Important properties 3- Transmission & Epidemiology 4- Pathogenesis & Immunity 5- Clinical Findings 6- Lab diagnosis & prevention 3
- 4. Hepatitis A is an acute infectious disease of the liver caused by the Hepatitis A virus There are Five medically important viruses infect the liver 1- HAV 2- HBV 3- HCV 4- HDV 5- HEV 4
- 5. 5
- 6. *- HAV is a typical enterovirus related to picornavirus family , it has a single strand RNA genome and a nonenveloped icosahedral nucleocapsid and replicates in the cytoplasm *-Has one serotype, and there is no antigenic relationship to HBV or other hepatitis viruses 6
- 7. 7
- 8. *- HAV is transmitted by the fecal–oral route and viruses appear in the stool 2 weeks before the appearance of symptoms, *- Children are the most common infected group . And mostly occurs in summer camps and boarding schools *- Sources of this virus arise from fecally contaminated water and eating raw foods .. (( it is unlike HBV & HCV ) *- 50 – 75 % of the adults in the united states are infected by this virus 8
- 9. *-pathogenesis of HAV isn't completely understood and infected hepatocytes usually produce no cytopathic effects . ( it occurs by the attack of the cytotoxic T cells ) *- No chronic infection after Hepatitis A ensues *-The immune response consists initially of IgM antibody which is detectable at the time of jaundice *- appearance of IgM is followed 1 to 3 weeks later by the production of IgG antibody which provides lifelong protection 9
- 10. The clinical manifestations of hepatitis are virtually the same . It includes Fever, anorexia, nausea, vomiting, and jaundice are typical *-Dark urine, pale feces, and elevated transaminase levels are seen *-Most cases resolve spontaneously in 2 to 4 weeks , and it has an incubation period of (3–4 weeks( *-There is no predisposition to hepatocellular carcinoma 10
- 11. 11
- 12. 1- The detection of IgM antibody is the most important test 2- A four-fold rise in IgG antibody titer can also be used. 3-isolation of the virus in cell culture is possible but not available in the clinical laboratory. 12
- 13. 1-active immunization with a vaccine containing inactivated HAV is available. . 2-passive immunization should be given to provide immediate protection and the vaccine given to provide long-term protection 3-vaccine is also effective in post-exposure prophylaxis if given within 2 weeks of exposure. 4-Twinrix vaccine can be given 5-proper hygiene (e.g sewage disposal and handwashing 13
- 14. 14
- 15. PRESENTED BY : SADI YEHIA NKAHALA SUPERVISED BY : DR : SAID ALGHORA
- 17. What a nice virus ! 17
- 18. HEPATITIS B VIRUS Disease HBV causes hepatitis B. Important Properties 1-HBV is a member of the Hepadnavirus family. (DNA enveloped virus ) 2-It is an enveloped virion with an icosahedral nucleocapsid core containing a partially double-stranded circular DNA genome 18 Hepatitis B Virion : Also known as a Dane particle (named for the scientist who first published electron micrographs of the virion).
- 19. Figure 41–1 19 FIGURE 41–2 Hepatitis B virus—electron micrograph. Long arrow points to a typical virion of hepatitis B virus. Short arrow points to a small sphere (just left of arrowhead) and a long rod (just right of arrowhead), both composed only of HB surface antigen
- 20. MCQ : Which of these organisms is also called Dane particle : 1-infectious HAV 2-infectious HBV 3-infectious HDV 4-infectious HCV 5-1+2+3 6-4+3+1 7-None of the above 8-all of the above 20
- 21. Table 41–2 21
- 22. HEPATITIS B VIRUS ((Electron microscopy of a patient’s serum reveals three different types of particles: a few virions and many spheres and long filaments which are composed of surface antigen (Figure 41–2). HBV is the only human virus that produces these spheres and filaments in such large numbers in the patient’s blood. The ratio of filaments and small spheres to virions is 1000:1)) 22
- 23. HEPATITIS B VIRUS The envelope contains a protein called the surface antigen (HBsAg), which is important for laboratory diagnosis and immunization. The genome contains four genes that encode five proteins <<: 1- the S gene encodes the surface antigen, 2- the C gene encodes the core antigen and the e antigen, 3- the P gene encodes the polymerase, 4- and the X gene encodes the X protein. The X protein is an activator of viral RNA transcription. 23 HBsAg was known as Australia antigen because it was first found in the serum of an Australian aborigine.
- 24. HEPATITIS B VIRUS In addition to HBsAg, there are two other important antigens: the core antigen (HBcAg) and the e antigen (HBeAg). The core antigen, as the name implies, forms the nucleocapsid core of the virion, the e antigen is secreted from infected cells into the blood. The e antigen is an important indicator of transmissibility. ) 24
- 25. HEPATITIS B VIRUS For vaccine purposes, HBV has one serotype based on HBsAg. The specificity of HBV for liver cells is based on two properties: 1-virus-specific receptors located on the hepatocyte cell membrane (facilitate entry) 2-transcription factors found only in the hepatocyte that enhance viral mRNA synthesis Humans are the only natural hosts of HBV. There is no animal reservoir. 25
- 26. Transmission & Epidemiology The three main modes of transmission are: 1- blood 2- sexual intercourse, 3- perinatally from mother to newborn. The observation that needle-stick injuries can transmit the virus indicates that only very small amounts of blood are necessary. HBV infection is especially prevalent in addicts who use intravenous drugs. Screening of blood for the presence of HBsAg has greatly decreased the number of transfusion-associated cases of hepatitis B 26
- 27. However, because blood transfusion is a modern procedure, there must be another, natural route of transmission. It is likely that sexual transmission and transmission from mother to child during birth or breast feeding are the natural routes. Note that enveloped viruses, such as HBV, are more sensitive to the environment than nonenveloped viruses and hence are more efficiently transmitted by intimate contact (e.g., sexual contact). Nonenveloped viruses, such as HAV, are quite stable and are transmitted well via the environment (e.g., fecal–oral transmission). 27
- 28. Hepatitis B is found worldwide but is particularly prevalent in Asia. Globally, more than 300 million people are chronically infected with HBV, and about 75% of them are Asian. There is a high incidence of hepatocellular carcinoma (hepatoma) in many Asian countries. Immunization against HBV has significantly reduced the incidence of hepatoma in children. It appears that the HBV vaccine is the first vaccine to prevent a human cancer. 28
- 29. 29 The specificity of HBV for liver cells ? Tell me why ??
- 30. Pathogenesis & Immunity 30 Pathogenesis Mainly by cell- mediated immunity Some symptoms occur as a result of Ag-Ab complex
- 31. Pathogenesis & Immunity After entering the blood, the virus infects hepatocytes, and viral antigens are displayed on the surface of the cells. Cytotoxic T cells mediate an immune attack against the viral antigens, inflammation and necrosis occur. Immune attack against viral antigens on infected hepatocytes is mediated by cytotoxic T cells. The pathogenesis of hepatitis B is probably the result of this cell-mediated immune injury, because HBV itself does not cause a cytopathic effect. Antigen–antibody complexes cause some of the early symptoms (e.g., arthralgias, arthritis, and urticaria) and some of the complications in chronic hepatitis (e.g., glomerulonephritis, cryoglobulinemia, and vasculitis). 31
- 32. 32
- 33. Pathogenesis & Immunity About 5% of patients with HBV infection become chronic carriers; in contrast, there is no prolonged carrier state in patients with HAV infection. A chronic carrier is someone who has HBsAg persisting in their blood for at least 6 months. The chronic carrier state is attributed to a persistent infection of the hepatocytes, which results in the prolonged presence of HBV and HBsAg in the blood. The main determinant of whether a person clears the infection or becomes a chronic carrier is the adequacy of the cytotoxic T-cell response. HBV DNA exists primarily as an episome in the cytoplasm of persistently infected cells; a small number of copies of HBV DNA are integrated into cell DNA. 33
- 34. What is ( episome ?) extra-chromosomal genetic material that may replicate autonomously or become integrated into the chromosome 34
- 35. Pathogenesis & Immunity A high rate of hepatocellular carcinoma occurs in chronic carriers. The HBV genome has no oncogene, and hepatocellular carcinoma appears to be the result of persistent cellular regeneration that attempts to replace the dead hepatocytes. Alternatively, malignant transformation could be the result of insertional mutagenesis, which could occur when the HBV genome integrates into the hepatocyte DNA. Integration of the HBV DNA could activate a cellular oncogene, leading to a loss of growth control. 35
- 36. Pathogenesis & Immunity Chronic carriage is more likely to occur when infection occurs in a newborn than in an adult, probably because a newborn’s immune system is less competent than that of an adult’s. Approximately 90% of infected neonates become chronic carriers. Chronic carriage resulting from neonatal infection is associated with a high risk of hepatocellular carcinoma. 36
- 37. Pathogenesis & Immunity Lifelong immunity occurs after the natural infection and is mediated by humoral antibody against HBsAg. Antibody against HBsAg (HBsAb) is protective because it binds to surface antigen on the virion and prevents it from interacting with receptors on the hepatocyte. (HBsAb is said to neutralize the infectivity of HBV.) Note that antibody against the core antigen (HBcAb) is not protective because the core antigen is inside the virion and the antibody cannot interact with it. 37
- 38. Lab Diagnosis ( serology) (enzyme ,, antigens ,, viral DNA ) 38 detectability
- 39. The window period lies between the end of detecting of surface antigen and the beginning of detecting the surface antigen -antibody 39
- 40. In window period ,, the amount of the surface antigens equal the amount of the surface antibody and u can not detect them in the blood 40 LOOK FOR HBC-AB
- 41. Lab Diagnosis ( serology) 41
- 42. In chronic Hepatitis B ,, we can not detect the surface antigen antibody as they will neutralize the surface antigens 42
- 43. 43
- 44. Laboratory Diagnosis The most important laboratory test for the detection of early HBV infection is the immunoassay for HBsAg. HBsAg appears during the incubation period and is detectable in most patients during the prodrome and acute disease 44
- 45. It falls to undetectable levels during convalescence in most cases; its prolonged presence (at least 6 months) indicates the carrier state and the risk of chronic hepatitis and hepatic carcinoma. HBsAb is not detectable in the chronic carrier state. Note that HBsAb is, in fact, being made but is not detectable in the laboratory tests because it is bound to the large amount of HBsAg present in the blood. HBsAb is also being made during the acute disease but is similarly undetectable because it is bound in antigen–antibody complexes. 45
- 46. Note that there is a period of several weeks when HBsAg has disappeared but HBsAb is not yet detectable. This is the window phase. At this time, the HBcAb is always positive and can be used to make the diagnosis. HBcAb is present in those with acute infection and chronic infection, as well as in those who have recovered from acute infection. Therefore, it cannot be used to distinguish between acute and chronic infection. The IgM form of HBcAb is present during acute infection and disappears approximately 6 months after infection. The test for HBcAg is not readily available. 46
- 47. HBeAg arises during the incubation period and is present during the prodrome and early acute disease and in certain chronic carriers. Its presence indicates a high likelihood of transmissibility, and, conversely, the finding of HBeAb indicates a lower likelihood, but transmission can still occur. DNA polymerase activity is detectable during the incubation period and early in the disease, but the assay is not available in most clinical laboratories. The detection of viral DNA (viral load) in the serum is strong evidence that infectious virions are present. 47
- 48. QUESTION 48
- 49. Answer 49
- 50. Prevention Prevention involves the use of either the vaccine or hyperimmuneglobulin or both. 50
- 51. Prevention (1) The vaccine (e.g., Recombivax) contains HBsAg produced in yeasts by recombinant DNA techniques. The vaccine is highly effective in preventing hepatitis B and has few side effects. The seroconversion rate is approximately 95% in healthy adults. It is indicated for people who are frequently exposed to blood or blood products, such as certain health care personnel (e.g., medical students, surgeons, and dentists), patients receiving multiple transfusions or dialysis, patients with frequent sexually transmitted disease, and abusers of illicit intravenous drugs. Travelers who plan a long stay in areas of endemic infection, such as many countries in Asia and Africa, should receive the vaccine. The U.S. Public Health Service recommends that all newborns and adolescents receive the vaccine 51
- 52. Prevention Seroconversion is the term used to describe the finding of antibody to a virus (or any microbe) in a patient’s serum when the patient previously had no antibody 52
- 53. Prevention At present, booster doses after the initial three-dose regimen are not recommended. However, if antibody titers have declined in immunized patients who are at high risk, such as dialysis patients, then a booster dose should be considered. Widespread immunization with the HBV vaccine has significantly reduced the incidence of hepatocellular carcinoma in children. A vaccine called Twinrix that contains both HBsAg and inactivated HAV provides protection against both hepatitis B and hepatitis A. 53
- 54. Prevention (2) Hepatitis B immune globulin (HBIG) contains a high titer of HBsAb. It is used to provide immediate, passive protection to individuals known to be exposed to HBsAg positive blood (e.g., after an accidental needle-stick injury). 54
- 55. Prevention Precise recommendations for use of the vaccine and HBIG are beyond the scope of this book. However, the recommendation regarding one common concern of medical students, the needle-stick injury from a patient with HBsAg-positive blood, is that both the vaccine and HBIG be given (at separate sites). This is true even if the patient’s blood is HBeAb positive. Both the vaccine and HBIG should also be given to a newborn whose mother is HBsAg-positive. These are good examples of passive–active immunization, in which both immediate and long-term protection are provided. All blood for transfusion should be screened for HBsAg. No one with a history of hepatitis (of any type) should donate blood, because non-A, non-B viruses may be present. 55
- 56. Thank You All 56
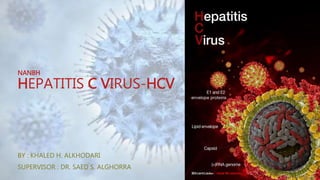
- 57. NANBH HEPATITIS C VIRUS-HCV BY : KHALED H.ALKHODARI SUPERVISOR : DR. SAED S.ALGHORRA
- 58. NON-A, NON-B HEPATITISVIRUSES-NANBH Describe the cases of hepatitis for which existing serologic tests had ruled out all known viral causes. The term is not often used because namely ,HCV, has been identified. 58
- 59. NANBH HCV was identified in 1989 after isolation of a viral RNA from a chimpanzee infected with blood from a person with NANBH.The viral RNA obtained from blood was converted to DNA with reverse transcriptase, its proteins were expressed, and antibodies from people with NANBH were then used to detect the viral proteins. These studies led to the development of ELISA and genomic and other tests for detection of the virus, which still cannot be grown in tissue culture 59
- 60. HEPATITIS C VIRUS Disease = HCV 60
- 61. IMPORTANT PROPERTIES A member of the flavivirus family. Enveloped virion. Genome (9100 nucleotides) encodes 10 proteins, Single-stranded Positivepolarity RNA. It has no virion polymerase. 61
- 62. IMPORTANT PROPERTIES At least six genotypes + multiple subgenotypes Based on differences in the genes that encode one of its two envelope glycoproteins “hypervariable” region in the envelope glycoprotein. Hypervariablety due to: The high mutation rate in the envelope gene The absence of a proofreading function in the virion-encoded RNA polymerase. So multiple subspecies (quasispecies) often occur in the blood of an infected individual at the same time. Genotypes 1a and 1b are the most common in the united states. 62
- 63. TRANSMISSION Humans are the reservoir for HCV. Transmitted primarily via blood. At present, injection drug use accounts for almost all new HCV infections. Transmission via blood transfusion rarely occurs? Transmission via needle-stick injury occurs, but the risk is < for HBV. Sexual transmission and transmission from mother to child occur but are inefficient modes. 63
- 64. World Hepatitis Day: July 28, 2015 64
- 65. 65
- 66. 66
- 67. EPIDEMIOLOGY 67
- 68. 68
- 69. 69
- 70. 70
- 71. TRANSMISSION & EPIDEMIOLOGY HCV is the most prevalent blood-borne pathogen in the U.S. In the nationally reported incidence HCV ranks below HIV and HBV as a blood- borne pathogen, but it is estimated that HCV is more prevalent. ~ 4 million people in the US (1%–2% of the population) are chronically infected with HCV. Unlike yellow fever virus, there is no evidence for an insect vector for HCV. Worldwide, it is estimated that 180m people are infected with HCV. 71
- 72. TRANSMISSION & EPIDEMIOLOGY In the united states, about 1% of blood donors have antibody to HCV. People who share needles when taking intravenous drugs are very commonly infected. Commercially prepared immune globulin preparations are generally very safe, but several instances of the transmission of HCV have occurred. This is the only example of an infectious disease transmitted by immune globulins.?? 72
- 73. PATHOGENESIS Infects hepatocytes primarily-how?-, no evidence for a cytopathic effect on it. Death of the hepatocytes is probably caused by immune attack by cytotoxic T cells. Strongly predisposes to hepatocellular carcinoma: But there is no evidence for: An oncogene in the viral genome Insertion of a copy of the viral genome into the DNA of the cancer cells. This supports the idea that the cancer is caused by prolonged liver damage and the consequent rapid growth rate of hepatocytes as the cells attempt to regenerate rather than by a direct oncogenic effect of HCV. Alcoholism greatly enhances the risk Patients with cirrhosis of any origin, not just alcoholic cirrhosis, have an increased risk 73
- 74. IMMUNITY Antibodies against HCV are made, but approximately 75% of patients are chronically infected and continue to produce virus for at least 1 year. Chronic carriage of HCV is much higher than the rate of chronic carriage of HBV. Chronic active hepatitis and cirrhosis occur in approximately 10% of these patients. For patients who clear the infection, it is not known whether reinfection can occur or whether there is lifelong immunity. 74
- 75. CLINICAL FINDINGS Acute infection with HCV is milder than infection with HBV. Fever, anorexia, nausea, vomiting, and jaundice are common. Dark urine, pale feces, and elevated transaminase levels are seen. Hepatitis C resembles hepatitis B as far as the ensuing chronic liver disease, cirrhosis, and the predisposition to hepatocellular carcinoma are concerned. Chronic carrier state occurs more often with HCV infection than with HBV. 75
- 76. CLINICAL FINDINGS Liver biopsy is often done in patients with chronic infection to evaluate the extent of liver damage and to guide treatment decisions. Many infections with HCV ,including both acute and chronic infections, are asymptomatic and are detected only by the presence of antibody. The mean incubation period is 8 weeks. Cirrhosis resulting from chronic HCV infection is the most common indication for liver transplantation. 76
- 79. CLINICAL FINDINGS HCV infection also leads to significant autoimmune reactions, including vasculitis, arthralgias, purpura, and membranoproliferative glomerulonephritis. The main cause of essential mixed cryoglobulinemia. composed of HCV antigens and antibodies. 79
- 80. LABORATORY DIAGNOSIS Detecting antibodies to HCV in an ELISA: ///What is known Ag or Ab ?? The antigen in the assay is a recombinant protein formed from three immunologically stable HCV proteins and does not include the highly variable envelope proteins. The test does not distinguish between IgM and IgG Does not distinguish between an acute, chronic, or resolved infection. False-positive results can occur in the ELISA. Confirmatory test= RIBA (recombinant immunoblot assay) + PCR that detects the presence of viral RNA (viral load) in the serum to determine whether active disease exists Isolation of the virus from patient specimens is not done. 80
- 81. 81
- 82. LABORATORY DIAGNOSIS A chronic infection is characterized by: Elevated transaminase levels A positive RIBA Detectable viral RNA For at least 6 months. 82
- 83. PREVENTION Blood found to contain antibody is discarded prevented virtually all cases of transfusion- acquired HCV infection since 1994, when screening began. There is no vaccine. Hyperimmune globulins are not available. Pooled immune serum globulins are not useful for postexposure prophylaxis. There is no effective regimen for prophylaxis following needle-stick injury; only monitoring is recommended. 83
- 84. PREVENTION HEPATOCELLULAR CARCINOMA Pt advised to reduce or eliminate their consumption of alcoholic beverages. Pt should be monitored with alpha-fetoprotein tests and liver sonograms. Pt with liver failure due to HCV infection can receive a liver transplant, but infection of the graft with HCV typically occurs. 84
- 85. 85
- 86. EPIDEMIOLOGIC AND CLINICAL FEATURES OFVIRAL HEPATITIS TYPES A, B,AND C 86
- 87. EPIDEMIOLOGIC AND CLINICAL FEATURES OFVIRAL HEPATITIS TYPES A, B,AND C 87
- 89. REFERENCES OF HEPATITIS CVIRUS WHO CDC 89
Editor's Notes
- The virus probably replicates in the gastrointestinal tract and spreads to the liver via the blood. The infection is cleared and the damage is repaired Uusually used in the lab diagnosis
- in contrast to that of HBV which is 10- 12 weeks هنا اقصد ال incubation period
- in contrast to that of HBV which is 10- 12 weeks هنا اقصد ال incubation period
- Two doses, an initial dose followed by a booster 6 to 12 months later, should be given. No subsequent booster dose is recommended. وهذا مثال ع passive- active immuinzation given to traveler to developing countries , to children between 2-18 and for men who have sex with men
- أهم ماركر للدلالة على وجود كرونيك انفكشين هو السيرفيس أنتجين بي اللي ضل لمدة ست شهور لكن كيف نميز بين الكرونيك و الكرونيك آكتيف ؟ عن طريق e-antigen Ab for e-antigen ازا كان عندك سيجيفيكانت إي أنتيجين مع البي يعني كرونيك اكتيف إي أنتي بادي يعني دخلت في كرونيك الكور أنتيجين بيعلي في الأكيوت و الكرونيك مش هيفيدك كتيرwindow : the amount of the surface antigens equal the amount of the surface antibody and u can not detect them in the blood في الويندو بيريود ,, بتروح تفحص للمريض ,, الأنتي كور , انت فحصت السيرفيس أنتيجين و السيرفيس أنتي بادي و لقيتهم نورمال و قلت للمريض متخافش يا حج ,, انت بخير يا غالي في الأكيوت هيباتايتيس , أول اتنين برتفعو هم : سيرفيس أنتيجين ,, و الإي انتيجين , و بيرتفع أيضاً الأنتي كور أنتي بادي في الأكيوت هيباتايتيس ما بتقدر تطلع لا على السيرفيس أنتيجين و لا على الأنتي بادي سيرفيس , بتطلع على الأنتي كور في الاكيوت هيباتايتيس , لما يظهر عندنا الأنتي سيرفيس أنتجين يعني انت في الكافاري موود هلأ في الكرونيك رحنا فحصنا السيرفس أنتجين و لقيناهم كانو مرتفعين خلال الست شهور اللي فاتت خلاص انت كرونيك للتمييز بين الكرونيك آكتيف و الكرونيك حاف بنطلع على الإي أنتيجين ,, في الكرونيك لا يوجد أنتي بادي للسيرفيس أنتجين لكن يوجد أنتي بادي للكور أنتيجين و يوجد أنتي بادي ل الإي أنتجين و كلاهما ما لهم غير اهمية واحدة و هي انو انت معك كرونيك هيباتايتس بي
- Within the core is a DNA-dependent DNA polymerase. The genome contains four genes (four open reading frames) that encode five proteins, namely, the S gene encodes the surface antigen, the C gene encodes the core antigen and the e antigen, the P gene encodes the polymerase, and the X gene encodes the X protein. The X protein is an activator of viral RNA transcription. The DNA polymerase has both RNA-dependent (reverse transcriptase) and DNA-dependent activity يوجد عندنا إيرلي ستيج لصناعة البروتين و ليت ستيج , هلأ هادا الفايروس بيستخدم الدي أن إيه ديبيندانت بولي ميريز عشان يروح يكمل الديفيكتيف بارتكل تبعون و يصير كومبليت دابل ستراند ,, و بعدها يتم تصنيع بروتين , من ضمن البروتينات اللي بيتم تصنيعها في المرحلة الاولى هي بروتين إكس , بعدها هادا البروتين بيحفز تكوين البروتيانات الاخرى في الليت فيز
- However, for epidemiologic purposes, there are four serologic subtypes of HBsAg based on a group-specific antigen, “a,” and two sets of mutually exclusive epitopes, d or y and w or r. This leads to four serotypes—adw, adr, ayw, and ayr—which are useful in epidemiologic studies because they are concentrated in certain geographic areas.
- the main cause of non-A, non-B hepatitis,
- out
- The viral RNA-dependent RNA polymerase is error prone and generates mutations in the glycoprotein and other genes.
- because donated blood containing antibody to HCV is discarded
- cdc
- 3.234
- binds to CD81 (tetraspanin) surface receptors, which is expressed on hepatocytes and B lymphocytes, and can also coat itself with LDL / VLDL and then use the lipoprotein receptor to facilitate uptake into hepatocytes.
- aNonicteric hepatitis is common in children.bAmong the age group 15–29 years, hepatitis B and C are often associated with drug abuse or promiscuous sexual behavior. Patients with transfusion-associated hepatitisB or C virus are generally older than age 29 years.