Downloaded 226 times

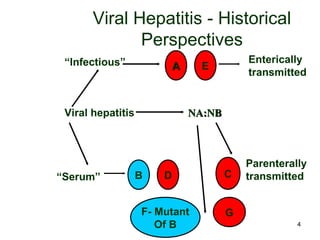
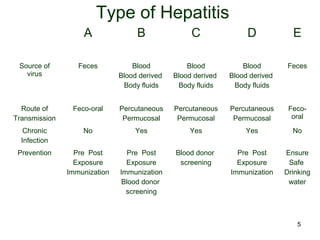
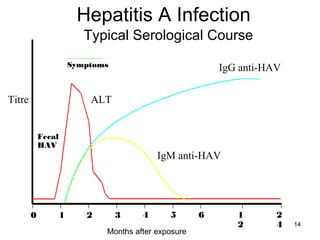
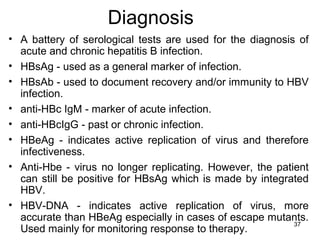
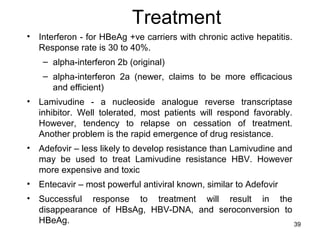
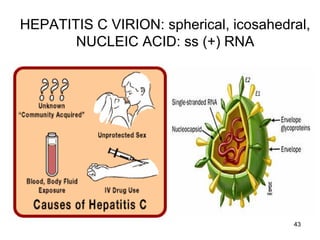
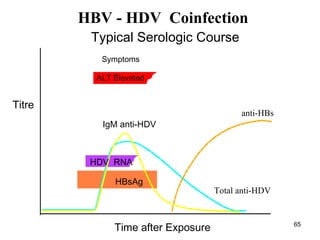
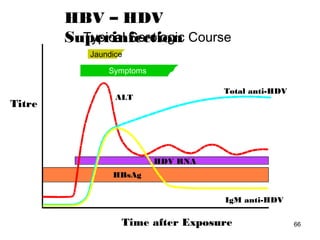


Hepatitis viruses include hepatitis A, B, C, D, and E. Hepatitis A virus is transmitted through the fecal-oral route while hepatitis B, C, and D are transmitted through blood and body fluids. Hepatitis B and C can cause chronic infections while hepatitis A usually does not. Diagnosis involves tests to detect viral antigens, antibodies, and nucleic acids. Treatment options depend on the hepatitis virus but may include antiviral drugs and vaccines to prevent transmission.























































































