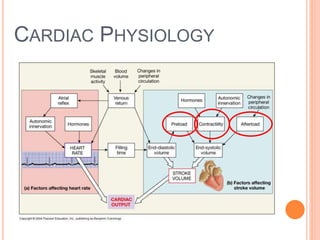
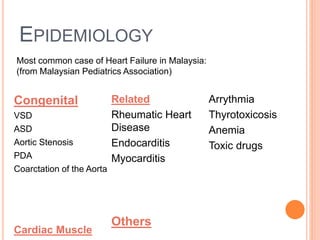
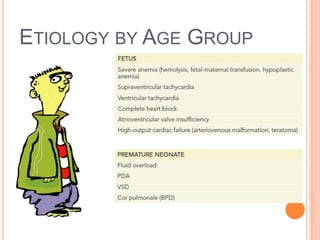
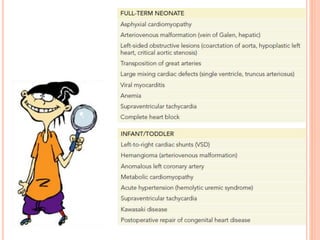
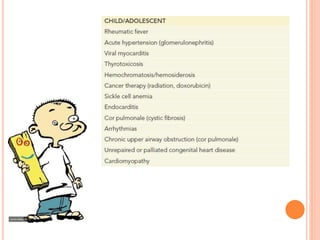
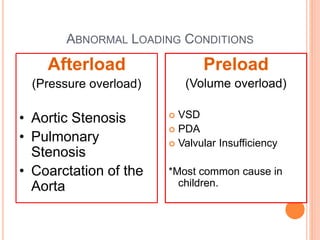
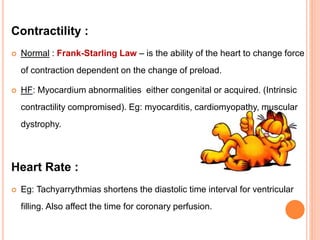
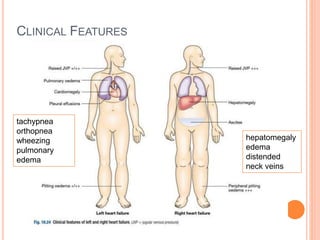
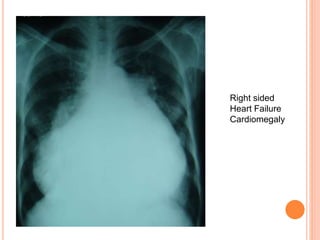
This document discusses heart failure in childhood. It defines heart failure as the heart's inability to deliver adequate cardiac output to meet the body's needs. The most common causes in children are congenital defects like VSD, ASD, or acquired conditions like rheumatic heart disease or myocarditis. Symptoms can include feeding difficulties, respiratory distress, or failure to thrive in infants. Diagnosis involves tests like echocardiogram, chest X-ray, and BNP levels to assess cardiac function and rule out other conditions. Treatment focuses on enhancing contractility, reducing preload and afterload, and improving oxygen delivery through medications, diuretics, and surgery or catheterization for congenital defects.