INTRODUCTION
•HF was describedas a clinical syndrome
caused by low cardiac output
characterized by typical symptoms and
signs associated with specific circulatory,
neurohormonal, and molecular
abnormalities
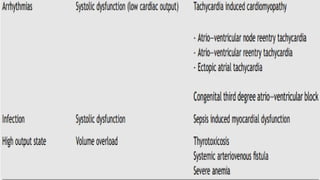
ETIOLOGY
•At birth, HFis caused by
•Fetal cardiomyopathies
•Extra cardiac conditions such as
•Sepsis
•Hypoglycemia
•hypocalcaemia
5.
ETIOLOGY
•In the 1stweek after birth
•CHDs with duct-dependent systemic
circulation such as
•severe aortic stenosis/aortic Coarctation
• hypoplastic left heart syndrome),
•closure of the ductus arteriosus causes
severe reduction of end-organ
perfusion,
6.
ETIOLOGY
•In the 1stmonth of life, frequent causes of HF are
•CHDs with left to right shunts
•VSDs
•patent ductus arteriosus
•aortopulmonary windows
•HF in adolescence is rarely secondary to CHDs, but is
more often related to cardiomyopathies, myocarditis,
RHD
10.
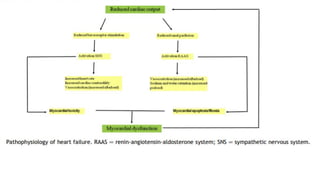
PATHOPHYSIOLOGY
•An “index event,”regardless of the cause,
produces an initial reduction of cardiomyocyte
contractility in HF
•The initial injury results in a reduction in
cardiac output that is, in turn, countered by
two major “compensatory mechanisms”
11.
PATHOPHYSIOLOGY CONT’
•Mechanisms include
•Activation of the sympathetic nervous system,
•resulting in increased release and decreased
uptake of norepinephrine, with peripheral
vasoconstriction to maintain (by increasing
systemic vascular resistance) mean arterial
pressure and organ perfusion.
PATHOPHYSIOLOGY CONT’
•Stimulation ofthe rennin - angiotensin aldosterone
system
•increased circulating levels of renin, angiotensin II,
and aldosterone
•Renin is responsible of cleaving angiotensinogen in
angiotensin I,
•Angiotensin I which is converted into angiotensin II
by the angiotensin-converting enzyme (ACE)
•Angiotensin II is a potent vasoconstrictor that
preserves end-organ perfusion.
14.
• Aldosterone causessalt and water retention
•Leads to increased preload and then cardiac output
according to the Franke Starling mechanism.
•However, the elevation of both aldosterone and
angiotensin II promotes cardiac fibrosis and apoptosis
• These mechanisms
•temporarily contribute to circulatory stability
•Over time become maladaptive and promote the
progression of HF
16.
CLINICAL FEATURES
•Older childrenand adolescence:
•Fatigue
•shortness of breath
•Tachypnea
•exercise intolerance are the main
symptoms.
CLINICAL FEATURES
•Infant andyoung children:
•The typical presentation is characterized by difficulty in
feeding (from prolonged feeding time intake to frank
intolerance)
•Cyanosis
•Tachypnea
•Sinus tachycardia
•Diaphoresis can be present.
Chest radiography
•Chest radiographyis indicated in all children
with suspected HF to assess
•heart size
•pulmonary edema
•Kerley B lines
•pleural effusions
Cardiac magnetic resonance
•Indicatedto study
•complex CHDs
•Tissue characterization
•Diagnosis
•risk-stratification, and ongoing management
of patients with specific forms of
cardiomyopathies
24.
Cardiac catheterization
•indicated for:
•Accurateevaluation of pressure gradients in
patients with complex valve diseases
•Evaluation of hemodynamic parameters
•Pulmonary and systemic vascular resistance
•Cardiac output, and cardiac index in Fontan
patients or during pre-transplant screening
25.
Labs
•Full blood count
•Usefulto assess anemia, which may
cause or aggravate heart failure
•Leukocytosis may result from stress or
signal an underlying infection
26.
Electrolytes
•Hyponatremia reflects anexpansion of
extracellular fluid volume in the setting of a
normal total body sodium
•Hypokalemia and hypochloremia can be the
result of prolonged administration of diuretics
27.
Electrolytes cont’
•Hyperkalemia canbe the result of
•impaired renal perfusion and marked
reductions in glomerular filtration
rate
•from intracellular potassium release
due to impaired tissue perfusion
•Hyperbilirubinemia (both directand indirect)
•is related to acute hepatic venous congestion and is
common with severe right heart failure.
•Elevated ALP, and prolongation of the PTT time can be
seen.
•In children with long-standing heart failure and poor
nutritional status
•hypoalbuminemia results from hepatic synthesis
impairment
TREATMENT
•Eliminate the causesof HF When possible, the causes
of HF must be corrected through different
approaches:
•corrective treatment should be performed in CHDs
•systemic diseases (such as sepsis)
•electrolytic imbalance (such as hypocalcemia) must
be carefully searched and treated.
34.
Treatment continues
•Control ofsymptoms and disease progression
•General measures
•In infants, nutritional support must ensure a caloric intake
about of 150 kcal/kg/d - small and frequent feeds
•Children and adolescents,25-30 kcal/kg/d
•Oxygen must be initiated when SaO2 < 90%.
• On the contrary, in patients with cyanotic CHD, oxygen has
little effect in raising SaO2 and MAY NOT BE indicated.
35.
TREATMENT CONT’
• Nursepropped up in a cardiac bed at an angle of
45o
• Strict bed rest
• Daily weight
• Daily urinalysis
• Reduction of salt intake is recommended
• Restriction of fluids
• Strict monitoring fluid input and output
36.
TREATMENT CONT’
•Medical therapy
•Focuseson three main goals:
•Decrease of pulmonary wedge pressure
•Increase of cardiac output and the
improvement of end organ perfusion
•Delay of disease progression
37.
TREATMENT CONT’
•Diuretics
•Diuretics therapyplays a crucial role in the treatment
of pediatric patients with HF.
•The benefits of diuretic therapy include
•Reduction of systemic, pulmonary, and venous
congestion
•Spironolactone may exert additional beneficial
effects by attenuating the development of
aldosterone-induced myocardial fibrosis and
catecholamine release.
38.
TREATMENT CONT’
•Potential complicationsof diuretic therapy include
•Electrolyte abnormalities (hyponatremia, hypo- or
hyperkaliemia, and hypochloremia)
•Metabolic alkalosis.
•Electrolyte balance should be carefully monitored,
especially during aggressive diuretic therapy
•failing myocardium is more sensitive to
arrhythmias induced by electrolyte imbalance.
39.
TREATMENT CONT’
• ACEinhibitors
• ACE inhibitors prevent, attenuate, or possibly reverse the
pathophysiological myocardial remodeling
• Decrease afterload by antagonizing the rennin-angiotensin
aldosterone
• Therapy with ACE inhibitors should be started at low doses with a
subsequent up-titration to the target dose with careful
monitoring of blood pressure, renal function, and serum
potassium.
40.
TREATMENT CONT’
• Betablockers
• Now an accepted therapy in the pediatric population
• Beta blockers
• Antagonize the deleterious effects of chronic sympathetic
myocardial activation and can reverse left ventricular remodeling
and improve systolic function
• Standard therapy may be useful in patients with left ventricular
systolic dysfunction
• Low-dose therapy should be started in stable patients with a
progressive up-titration to the target dose.
• Carvedilol often a good choice
41.
TREATMENT CONT’
•Inotropes
•Digoxin isthe main oral inotropic drug used in PHF
•Indicated in symptomatic patients with systolic dysfunction
•Results in improved cardiac output and blood pressure
•Final result is increased myocardial oxygen consumption
and demand.
•hemodynamic collapse can occur with high-dose inotropic
support
•Myocardium has a limited contractile reserve
42.
TREATMENT CONT’
• Sympathomimeticamines:
• Dopamine and dobutamine
• Effective inotropes and vasopressors in neonates, infants, and
children with circulatory failure.
• Increase cardiac output and decrease systemic and pulmonary
vascular resistance
• However, they can induce tachycardia/tachyarrhythmia with a
mismatch between myocardial oxygen delivery and the
requirement
• Therefore, they are drugs for patients with low cardiac output
despite other therapies
43.
TREATMENT CONT’
•Heart transplantation
•Acceptedtreatment for patients with refractory HF
•Cardiac transplantation significantly increases survival,
functional capacity, and quality of life
•Median survival in relation to age at the time of
transplantation
•19.7 years for infants
•16.8 years for children ages 1 - 5 years
•14.5 years for children ages 6 - 10 years
•12.4 years for children 11 - 17 years of