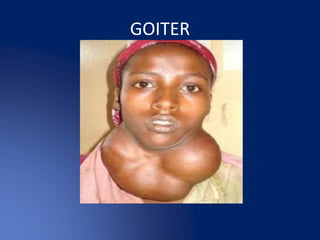
3. GOITER
The normal thyroid gland is impalpable. The term
goitre (from the Latin guttur = the throat) is used to
describe generalised enlargement of the thyroid
gland.
A discrete swelling (nodule) in one lobe with no
palpable abnormality elsewhere is termed an
isolated (or solitary) swelling.
7. Simple goiter
Aetiology
Simple goitre may develop as a result of stimulation of the
thyroid gland by TSH,
Inappropriate secretion from the anterior pituitary a
microadenoma
In response to a chronically low level of circulating thyroid
hormones.
1. The most important factor in endemic goitre is dietary
deficiency of iodine, Goitrogens in food.
8. Simple goiter
There is chronic deficiency of Thyroxine (T4) and or
triiodotrynine (T3) in the body which in turn causes
compensatory elevation of TSH because of the lack
of necessary negative feedback.
Prolonged stimulation of TSH in attempt to bring
normal thyroid hormones level leads to simple
goiter.
10. Pathophysiology
Chronic absence of T4/T3 causes elevated
level of TSH, which then leads to diffuse
hypertrophy and hyperplasia of follicular
cells and colloid (secretory follicles) in
efforts to produces more thyroid hormones.
11. Clinical presentation
Gradual onset of painless anterior neck
swelling, usually long standing in
endemically iodine deficient areas.
Recent onset of pain or increase in size may
indicate secondary changes.
13. Investigation in simple goiter
Thyroid function test
– thyroxine (T4),
– tri iodothyronine (T3),
– thyroid stimulating hormones (TSH)
• This helps to know if the thyroid gland is
normal, hyper or hypo functioning.
14. Thyroid scan with radioactive iodine
(I123 or I131)
• In this investigation a traceable radioactive Iodine or
Technetium is injected into the blood stream, the thyroid
gland concentrates radioactive iodine.
• I123 has a shorter half life as compared to I131 and therefore
preferred because it has less exposure of the patient to
radiation.
16. Thoracic inlet X-rays
may demonstrate
compression or
deviation of the
trachea, this
important to
anesthetist if surgery
is contemplated
(difficult intubation).
17. Computed tomography
may be indicated if
more details are
needed before surgery
or there is suspicion of
malignancy
transformation.
19. Treatment and prevention of simple
goiter
Dietary
• Iodine supplementation in iodine deficient
areas, food iodine fortification is one of the
best preventive measures of goiters.
Medical
Thyroxin supplementation
• In patients with diffuse hyperplastic goiter for
several months
20. Surgery indications
In patients with obstructive
symptoms,
When malignancy is suspected
clinically or after FNAC
For cosmetic reasons
21. Hypothyroidism is a condition
characterized by abnormally low
thyroid hormone production.
Because thyroid hormone affects
growth, development, and many
cellular processes, inadequate
thyroid hormone has widespread
consequences for the body.
HYPOTHYROIDSM
22. Medications and food (GOITROGENS)
Pituitary or hypothalamic disease
Severe iodine deficiency
Thyroid destruction (from radioactive iodine
or surgery)
Hashimoto's thyroiditis
Aetiology
24. In this condition, the thyroid gland is usually
enlarged (goiter) and has a decreased ability
to make thyroid hormones.
Hashimoto's is an autoimmune disease in
which the body's immune system
inappropriately attacks the thyroid tissue.
Hashimoto's thyroiditis
25. Increased antibodies to the enzyme, thyroid
peroxidase (anti-TPO antibodies).
Hashimoto's can be identified by detecting
anti-TPO antibodies in the blood
Hashimoto's thyroiditis
26. If for some reason the pituitary gland or the
hypothalamus are unable to signal the thyroid
and instruct it to produce thyroid hormones, a
decreased level of circulating T4 and T3 may
result, even if the thyroid gland itself is normal.
If this defect is caused by pituitary disease, the
condition is called "secondary hypothyroidism."
If the defect is due to hypothalamic disease, it is
called "tertiary hypothyroidism."
Pituitary or Hypothalamic disease
27. Fatigue
Depression
Modest weight gain
Cold intolerance
Excessive sleepiness
Dry, coarse hair
Constipation
Dry skin
Muscle cramps
Increased cholesterol
levels
Decreased
concentration
Vague aches and pains
Swelling of the legs
Common symptoms
28. • As the disease becomes more severe, there
may be puffiness around the eyes, a
slowing of the heart rate, a drop in body
temperature, and heart failure.
• In its most profound form, severe
hypothyroidism may lead to a life-
threatening coma (myxedema coma).
29. A diagnosis of hypothyroidism can be suspected
in patients with fatigue, cold intolerance,
constipation, and dry, flaky skin.
A blood test is needed to confirm the diagnosis.
When hypothyroidism is present, the blood levels
of thyroid hormones are usually decreased.
However, in early hypothyroidism, the level of
thyroid hormones (T3 and T4) may be normal.
Diagnosis of hypothyroidism
31. Cretinism
Clinical features:
Impaired skeletal development
Impaired CNS development
Inadequate maternal thyroid hormone prior to
fetal thyroid gland formation
SEVERE mental retardation
Normal brain development if maternal thyroid
deficiency occurs after fetal thyroid gland
development
32. Toxic goiter, thyrotoxicosis or
hyperthyroidism
Hyperthyroidism is a condition in which an overactive
thyroid gland is producing an excessive amount of
thyroid hormones that circulate in the blood.
Thyrotoxicosis can be caused by an excessive intake of
thyroid hormone or by overproduction of thyroid
hormones by the thyroid gland.
Hyperthyroidism can be primary or secondary
depending on the etiology.
33. Causes of hyperthyroidism
Graves' Disease
Functioning adenoma ("hot nodule") and
toxic multinodular goiter (TMNG)
Excessive intake of thyroid hormones
Abnormal secretion of TSH
Thyroiditis (inflammation of the thyroid
gland)
34. Primary hyperthyroidism
Grave’s disease
Graves’s disease is an autoimmune disease of
the thyroid gland, where there is an over-
production of the thyroid hormone which
causes enlargement of the thyroid and other
symptoms such as exophthalmos, heat
intolerance and anxiety.
35. In patients with secondary hyperthyroidism,
there is a pre existing thyroid pathology for
example multinodular goitre (occurs due to
hypertrophy and hyperplasia of gland
leading to excess production of thyroid
hormones).
Secondary hyperthyroidism
36. Inflammation of the thyroid gland may occur
after a viral illness (Subacute thyroiditis).
This condition is associated with a fever and a
sore throat that is often painful on swallowing.
The thyroid gland is also tender to touch.
There may be generalized neck aches and pains.
Inflammation of the gland with an accumulation
of white blood cells known as lymphocytes
(lymphocytic thyroiditis) may also occur.
Thyroiditis
37. Central nervous system
Central nervous system features are very
common in patients with primary
thyrotoxicosis.
tremors which can be observed on the tongue
and fingers,
nervousness,
emotional liability (patients become irritated
easily), they may also be lethargic or agitated
and usually they have warm and moist hands.
Clinical features of hyperthyroidism
38. Increased metabolic rate
weight loss,
heat intolerance,
excessive sweating, and
tiredness cause by muscle weakness
as a result of proteolysis.
39. Gastro intestinal tract (GIT);
loss of body weight despite having good or
increased appetite, and
increase bowel motions (diarrhea).
40. Genital urinary tract (GUT)
irregular menstruation,
amenorrhea,
loss of libido and
erectile dysfunctions
43. A rare presentation of thyrotoxicosis, there is extreme
signs of thyrotoxicosis associated with severe metabolic
disturbances.
It occurs in patient with hyperthyroidism who has not
been well prepared (hyperthyroidism is not controlled)
before surgery.
Clinical features includes;
hyper-thermia,
tachycardia,
irritability,
profuse sweating and
diarrhea.
Thyroid storm (thyrotoxic crisis)
44. • This targets central nervous system and
cardiovascular symptoms.
• Beta adrenergic blockers are the mainstay of
symptomatic therapy for thyrotoxicosis.
• Propranolol has benefit of inhibition of
peripheral conversion of T4 to T3
Symptomatic treatment
45. These drugs either blocks iodine binding to
tyrosine and decrease antibody titers
(Carbimazole) or block iodine binding and
prevent conversion of T4 to T3
(propylthiouracil).
Antithyroid treatment
47. All patients must be euthyroid before
embarking in surgery, ECG, CXR, and
Echocardiogram must be done to rule out
arrhythmia and heart failure.
Thoracic inlet X-ray in huge goiters to rule
tracheal deviation and compression as
discussed above.
Surgical treatment
48. Subtotal thyroidectomy; leaves about 8-10 gram
of thyroid tissue, either 4-5gram on each side or
8-10 gram on one side.
Near total thyroidectomy removes nearly all
thyroid tissue leaving only about 4gm thyroid
tissue
Lobectomy removes the entire lobe one side with
isthmusectomy eg in solitary toxic nodule
Types of surgery