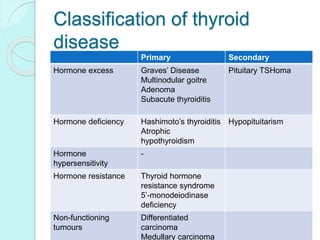
The document provides a comprehensive overview of thyroid diseases, highlighting their prevalence, types, and clinical features, with a specific focus on conditions such as goitre, thyroiditis, and various types of thyroid cancers. It details symptoms, diagnostic methods, and management strategies, including medication, surgery, and radioactive iodine treatment. The document underscores the gender disparities in thyroid diseases and emphasizes the importance of proper diagnosis and treatment options for thyroid-related conditions.