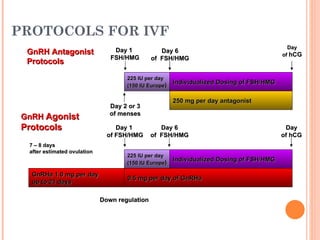
The document discusses changing protocols for in vitro fertilization (IVF) from gonadotropin-releasing hormone (GnRH) agonists to GnRH antagonists. Some key points discussed include:
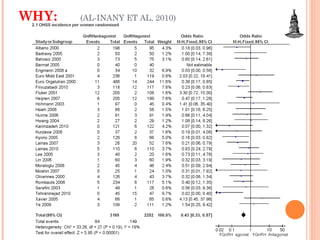
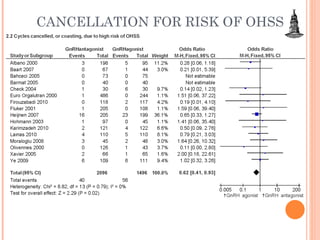
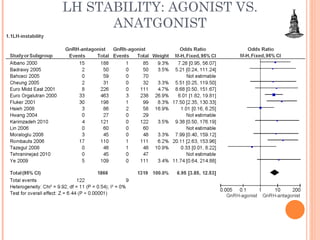
1) GnRH antagonists are associated with a lower risk of ovarian hyperstimulation syndrome (OHSS) compared to GnRH agonists.
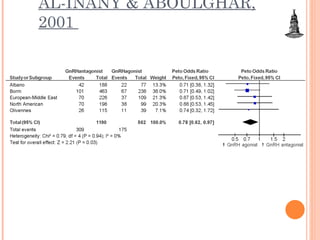
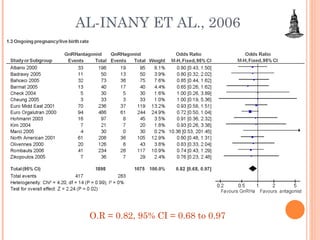
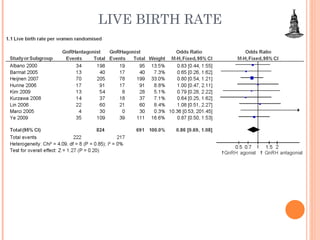
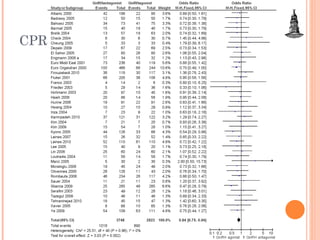
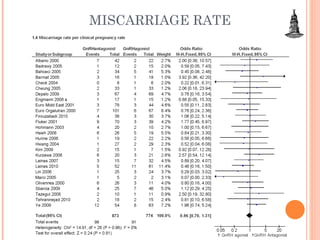
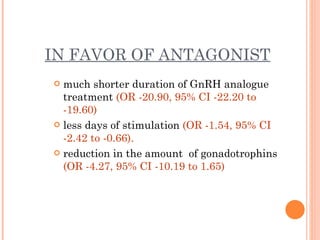
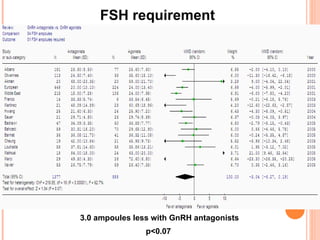
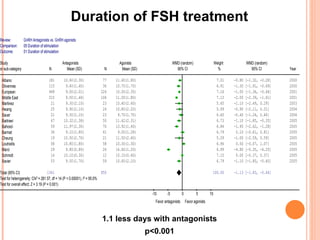
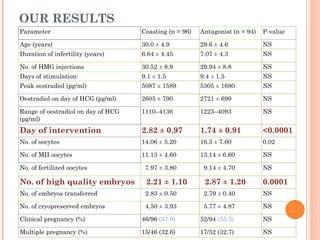
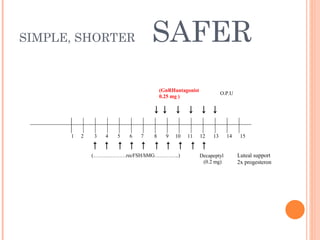
2) While efficacy outcomes like live birth and pregnancy rates are similar between the two protocols, GnRH antagonists require fewer gonadotropin ampoules and have a shorter duration of stimulation.
3) Based on multiple randomized controlled trials and meta-analyses, it is justified to shift from GnRH agonists to GnRH antagonists for IVF