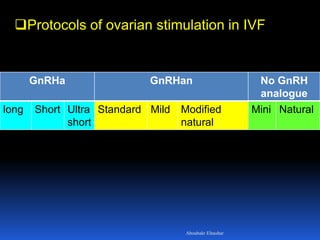


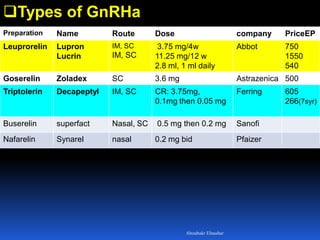
![Protocols
Ultra-short (sequential):
Based on
initial stimulatory effect of GnRHa on Gnt secretion
[flare- up effect]
lasts for 1-2 days
promotes simultaneous maturation of several
follicles.
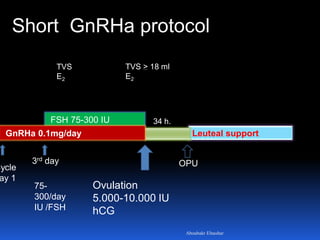
GnRHa: from the 1st to 3rd day of the cycle.
Gnt: from the 3rd day of the cycleAboubakr Elnashar](https://image.slidesharecdn.com/cos-copy-150101071510-conversion-gate02/85/Controlled-ovarian-stimulation-in-IVF-17-320.jpg)
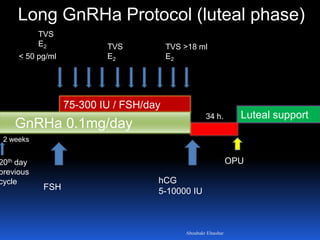
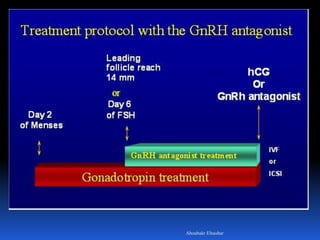
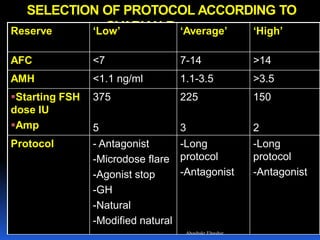

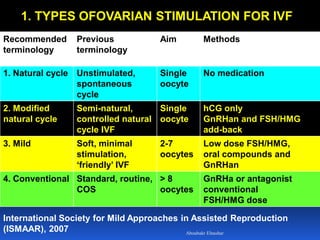
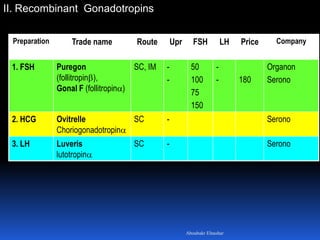
This document discusses different types of ovarian stimulation protocols used in IVF. It begins by describing 4 main types of stimulation: natural/modified natural cycles involving little to no medication; mild stimulation involving low dose FSH/HMG; conventional stimulation using standard FSH/HMG doses; and high stimulation. It then covers the drugs used for ovarian stimulation, including gonadotropins and GnRH analogues. The rest of the document discusses specific GnRH agonist and antagonist protocols, methods of triggering ovulation including hCG and GnRH agonists, and criteria for cycle cancellation.






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







