
Downloaded 75 times
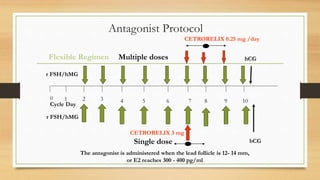
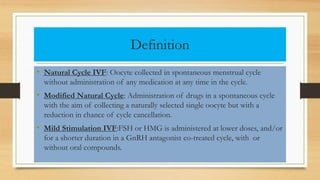
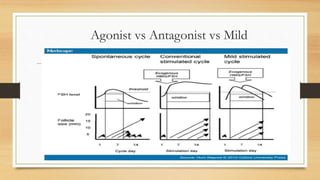
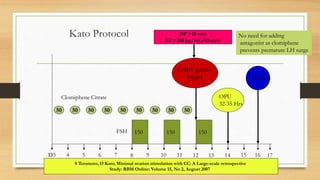
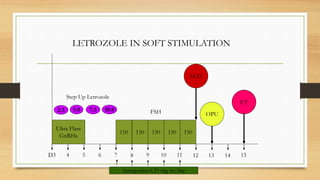
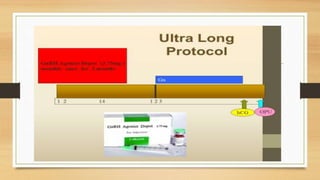

The document outlines various approaches to ovarian stimulation for ovulation induction, including controlled ovarian hyperstimulation (COS) and different medication protocols (agonist, antagonist, and mild stimulation). It emphasizes the importance of individualized treatment to optimize success rates in assisted reproductive technology while minimizing risks such as ovarian hyperstimulation syndrome (OHSS) and cycle cancellation. Comparisons are made between different stimulation protocols, highlighting their effectiveness and suitability for various patient profiles, particularly for those with diminished ovarian reserve or poor responders.



































































