Download as PDF, PPTX

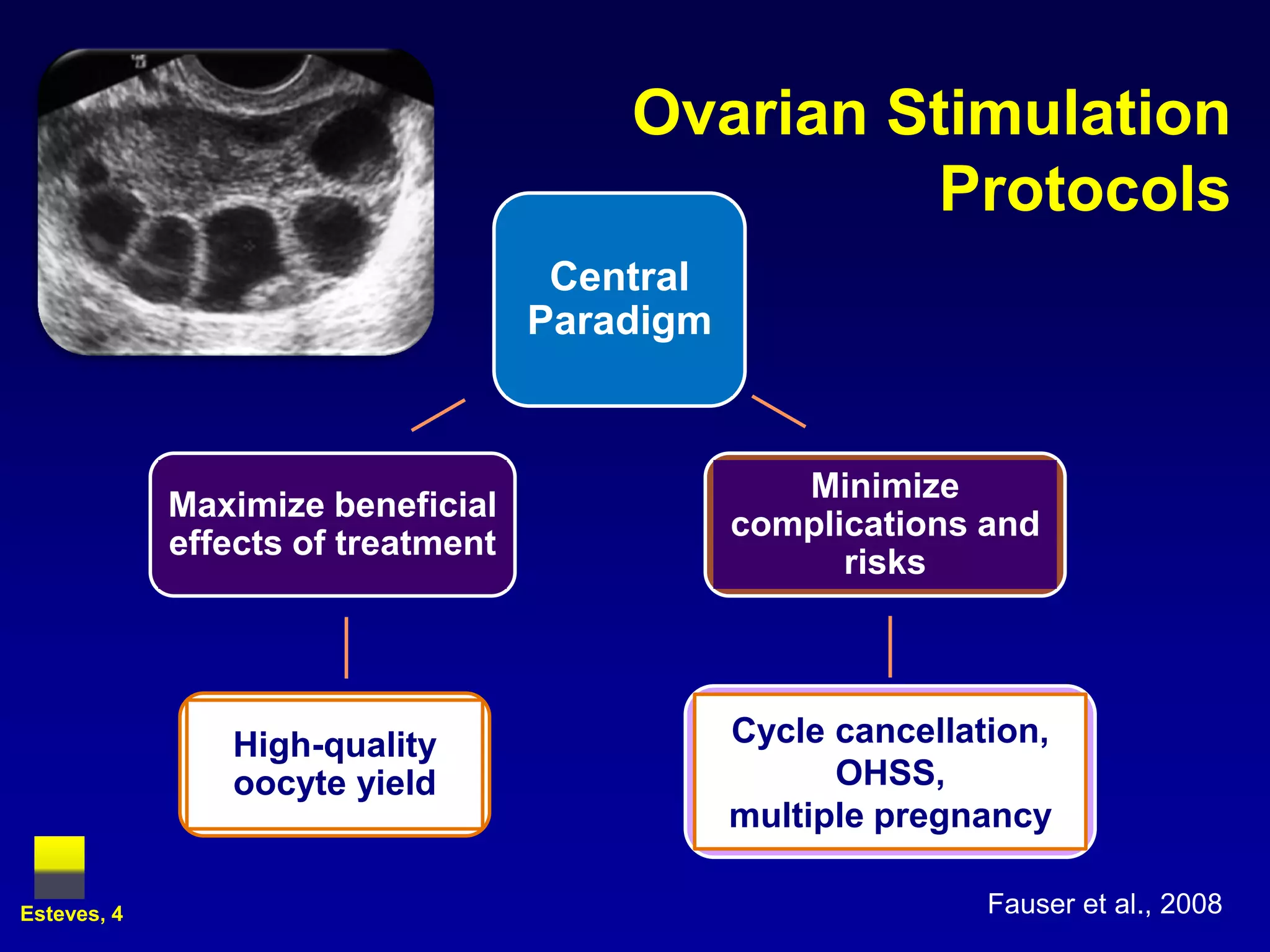
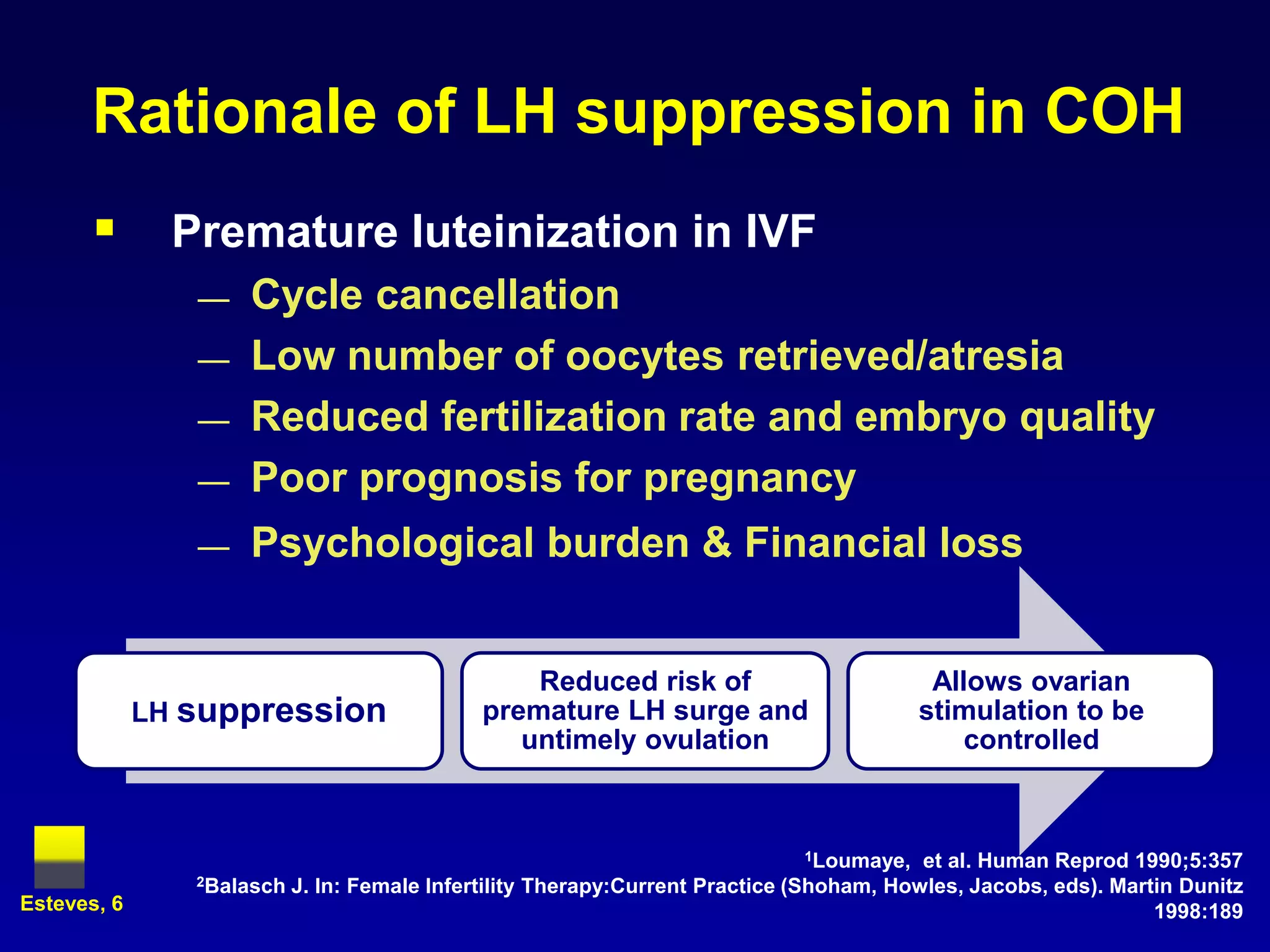
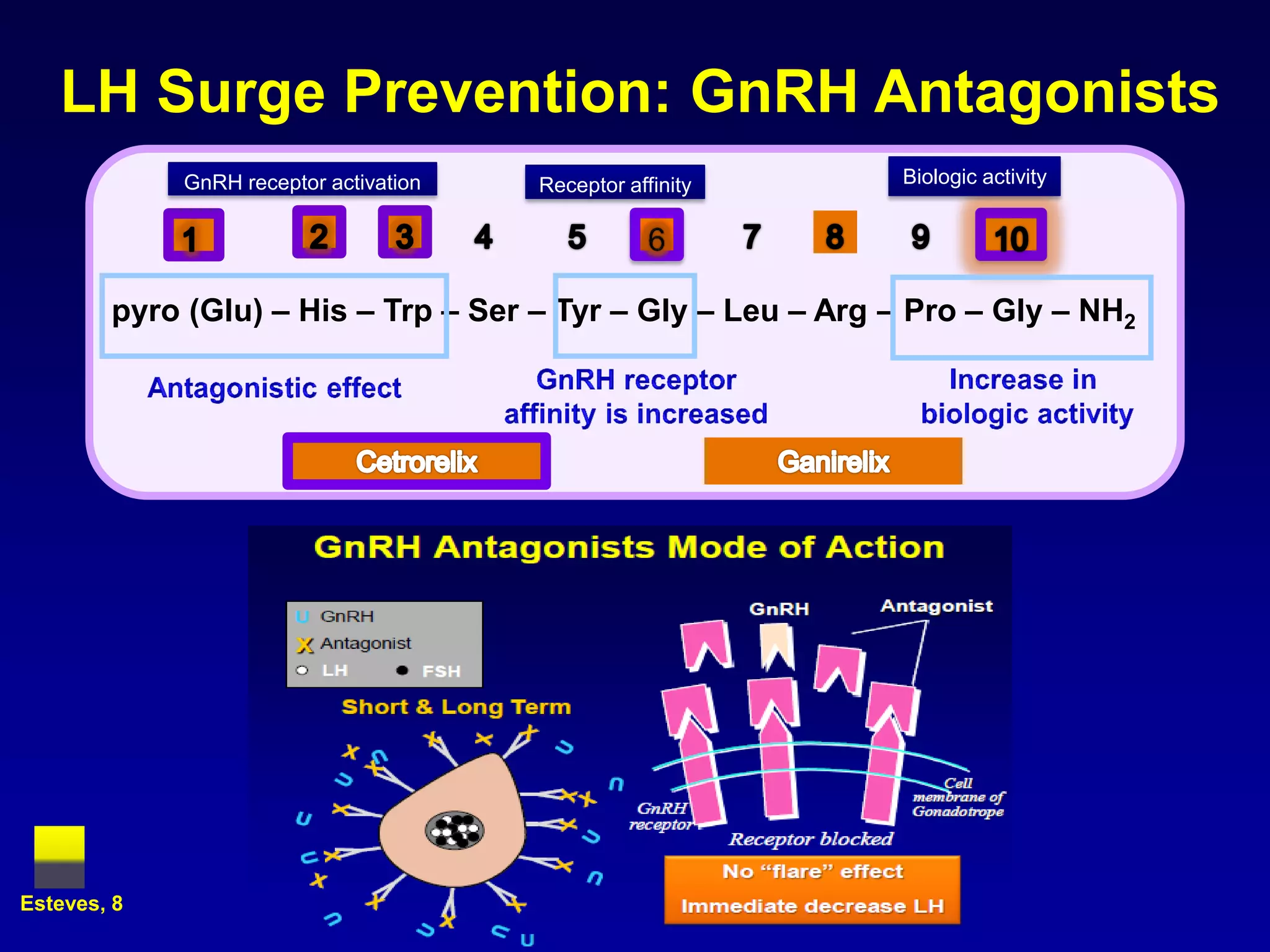
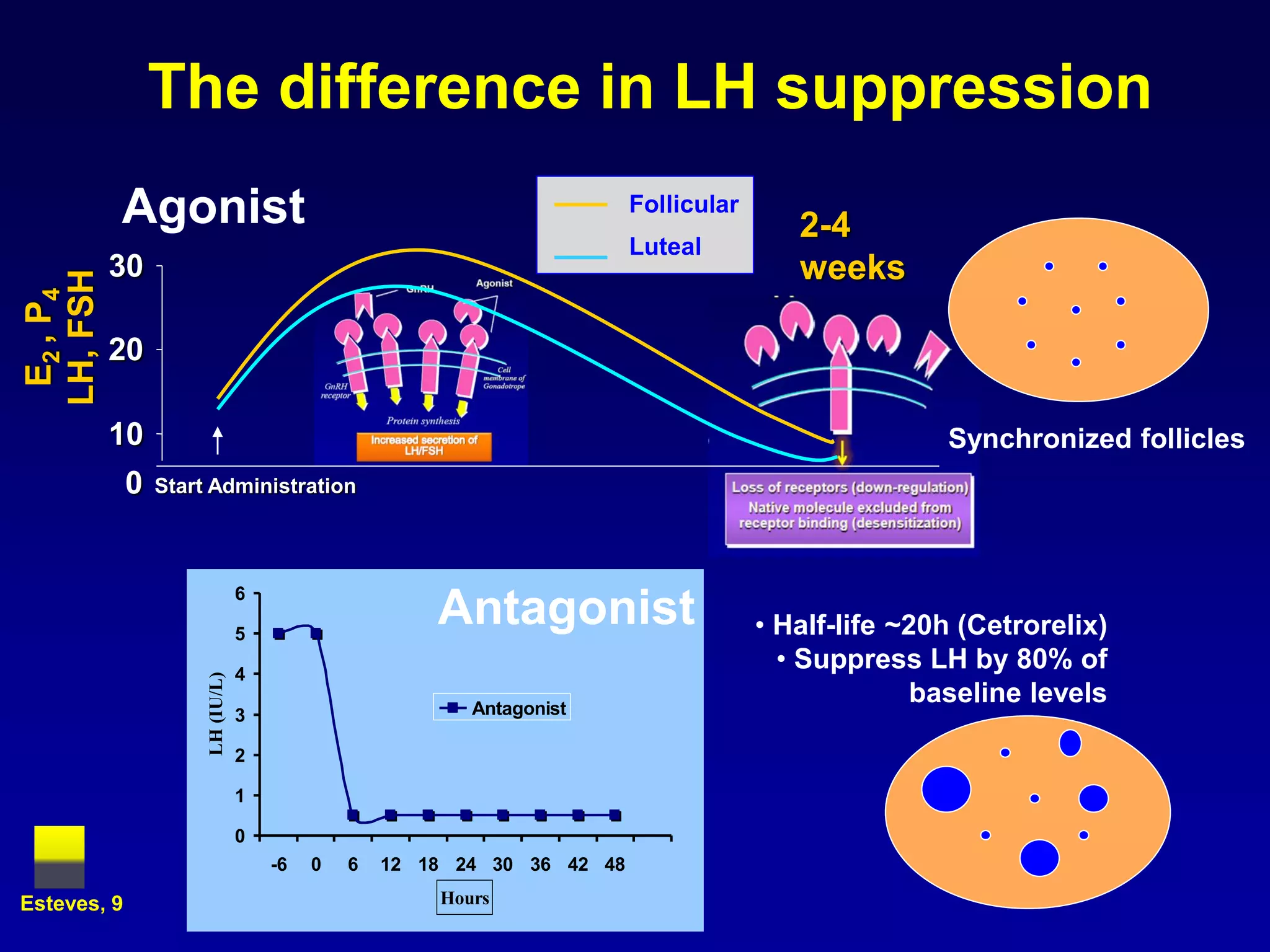
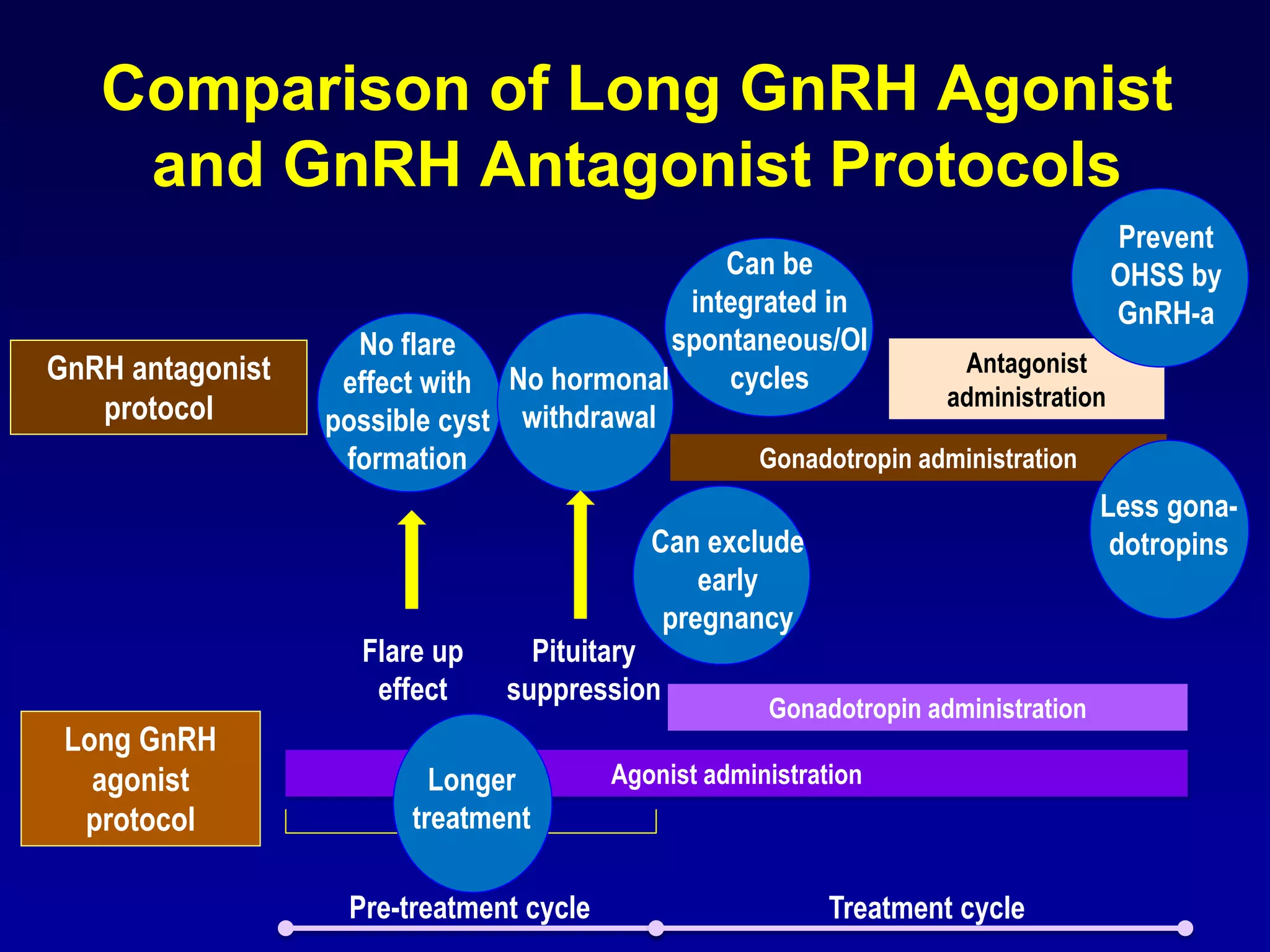
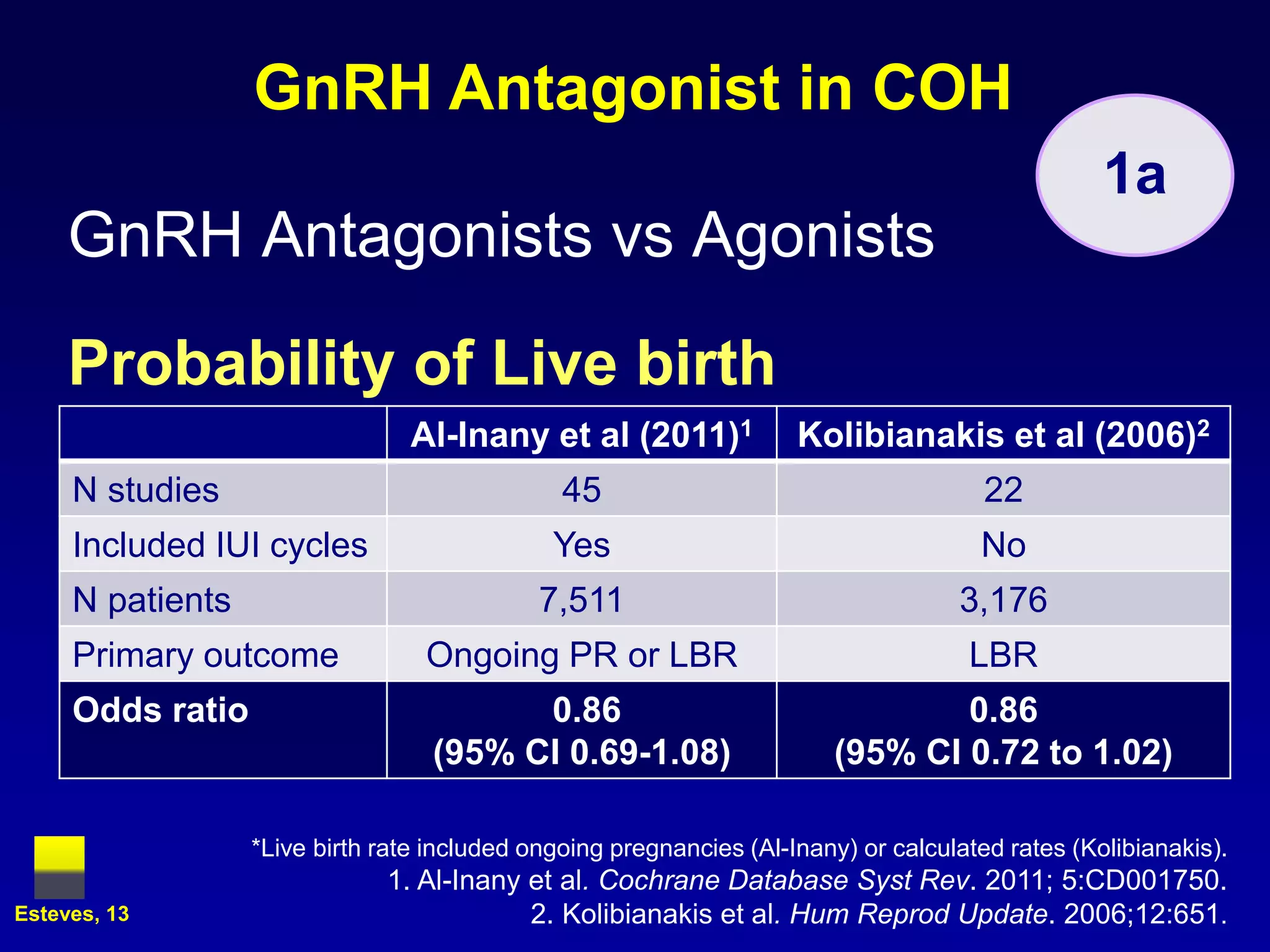
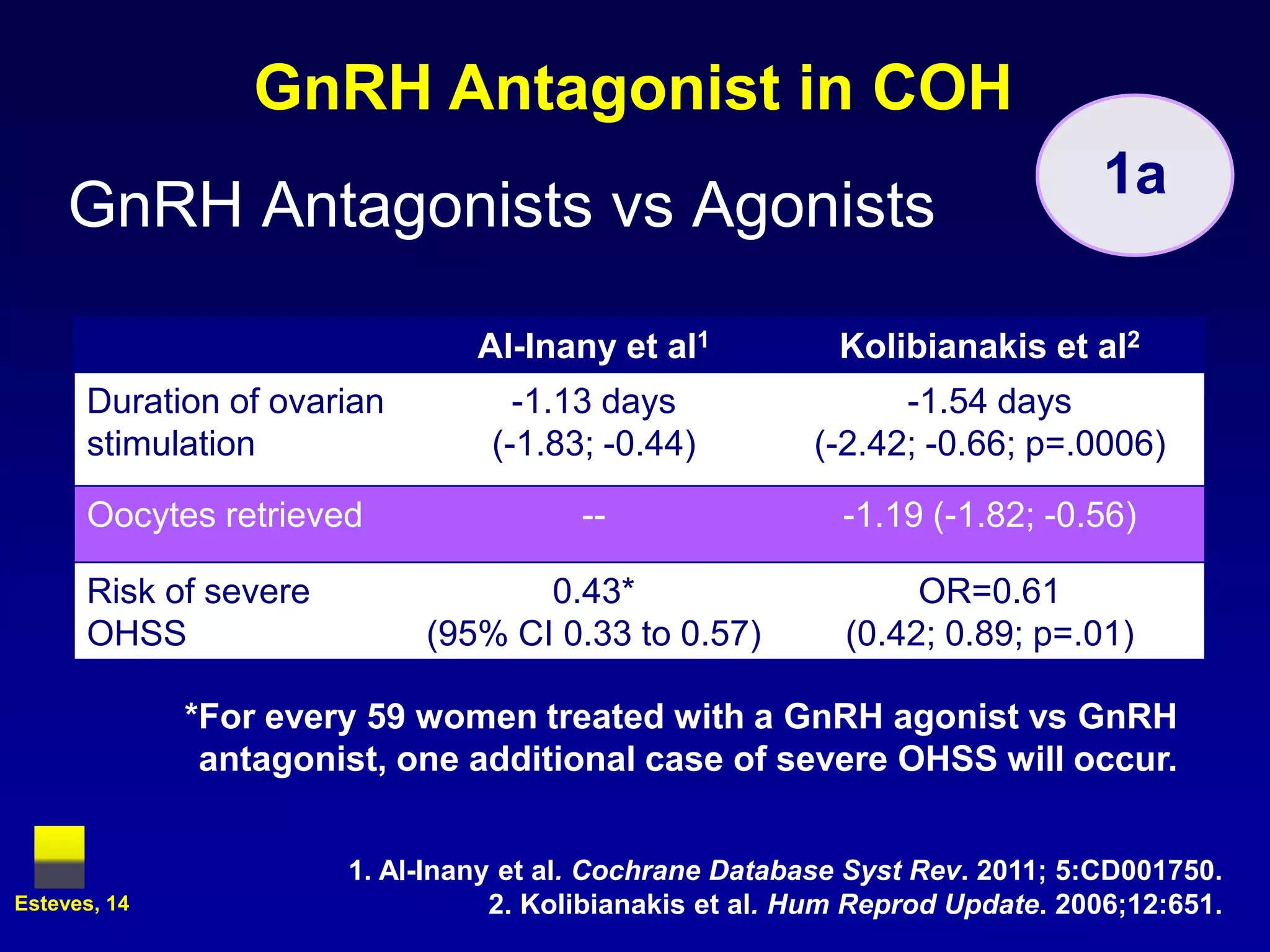
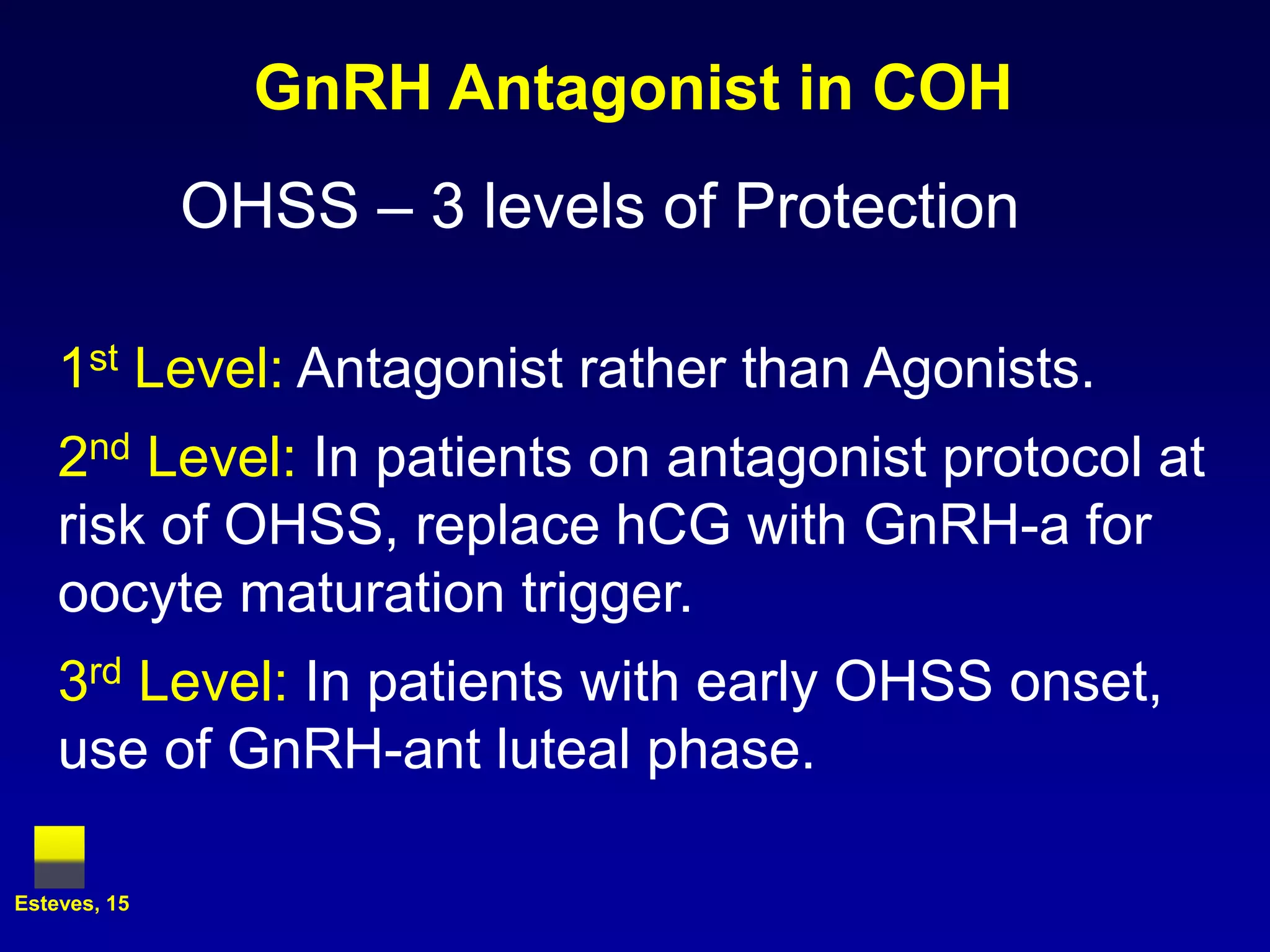
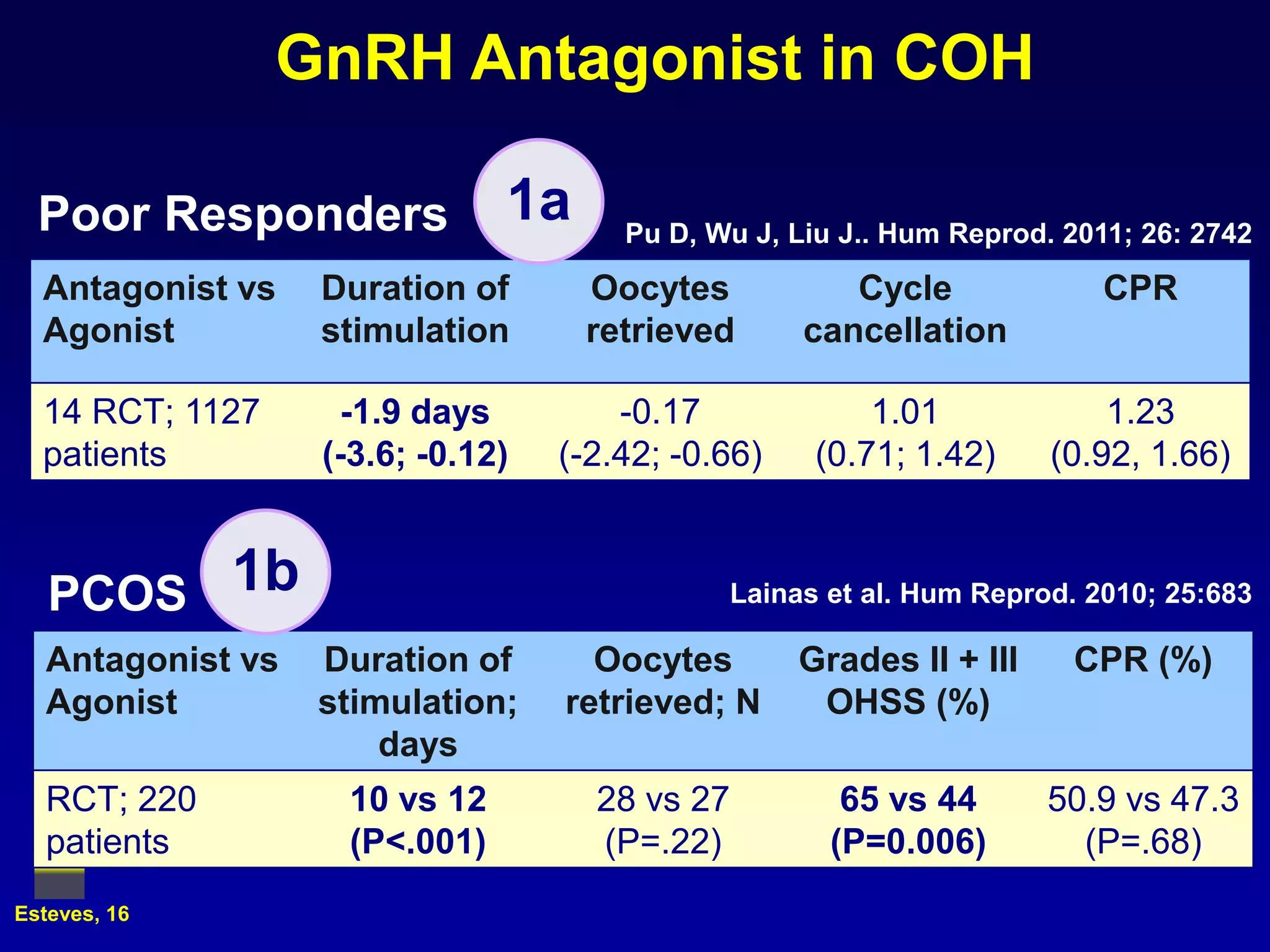
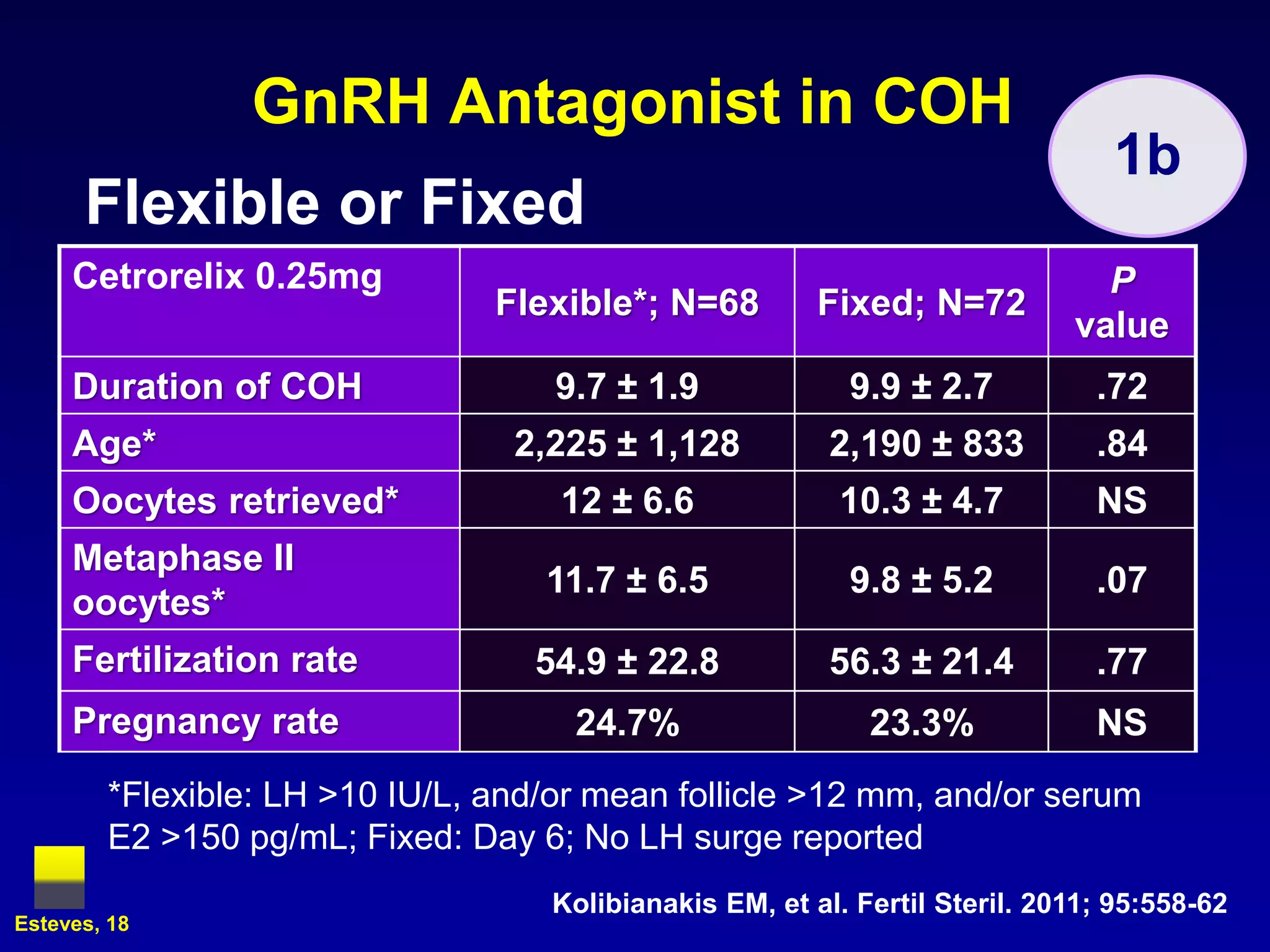
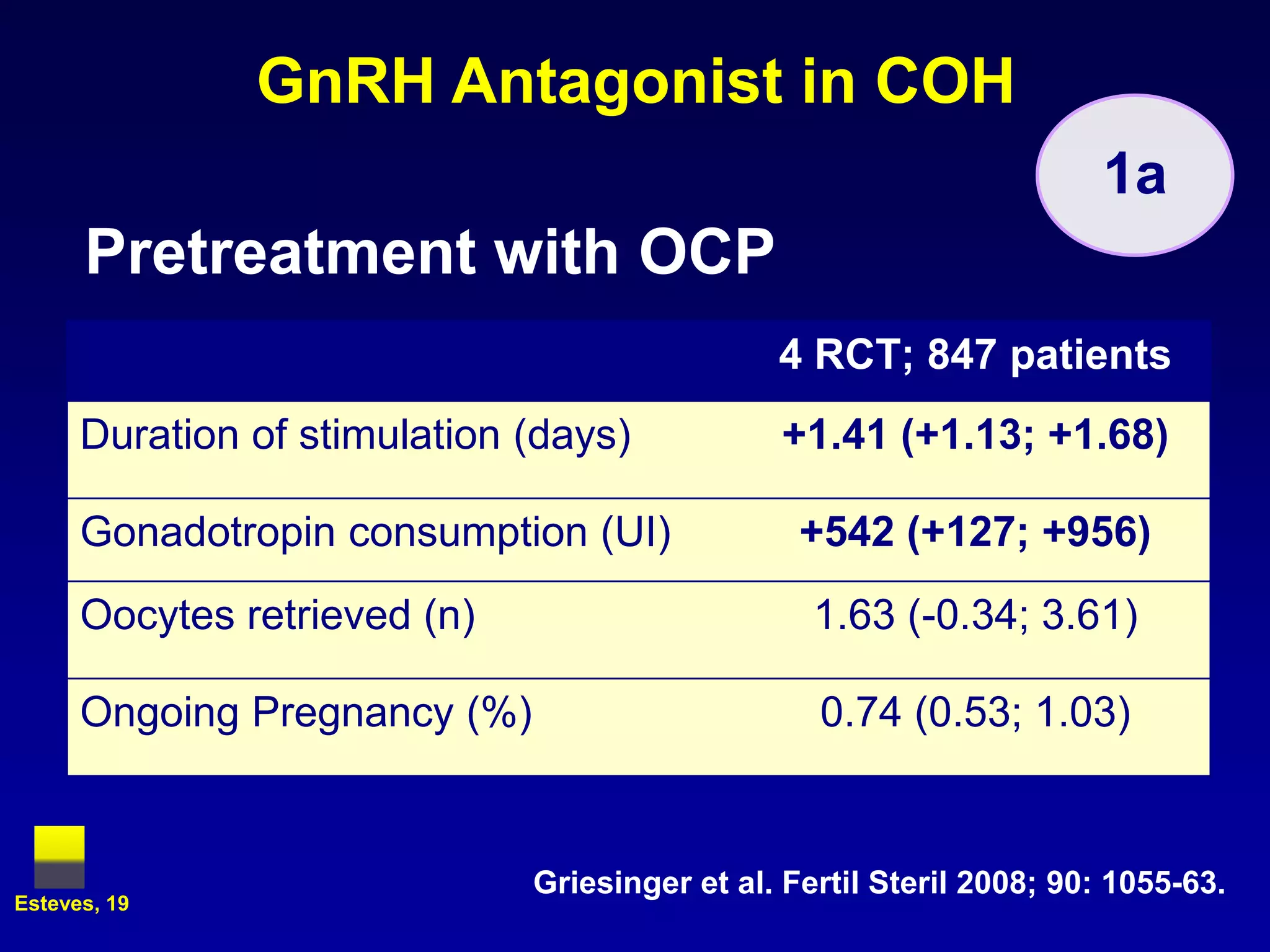
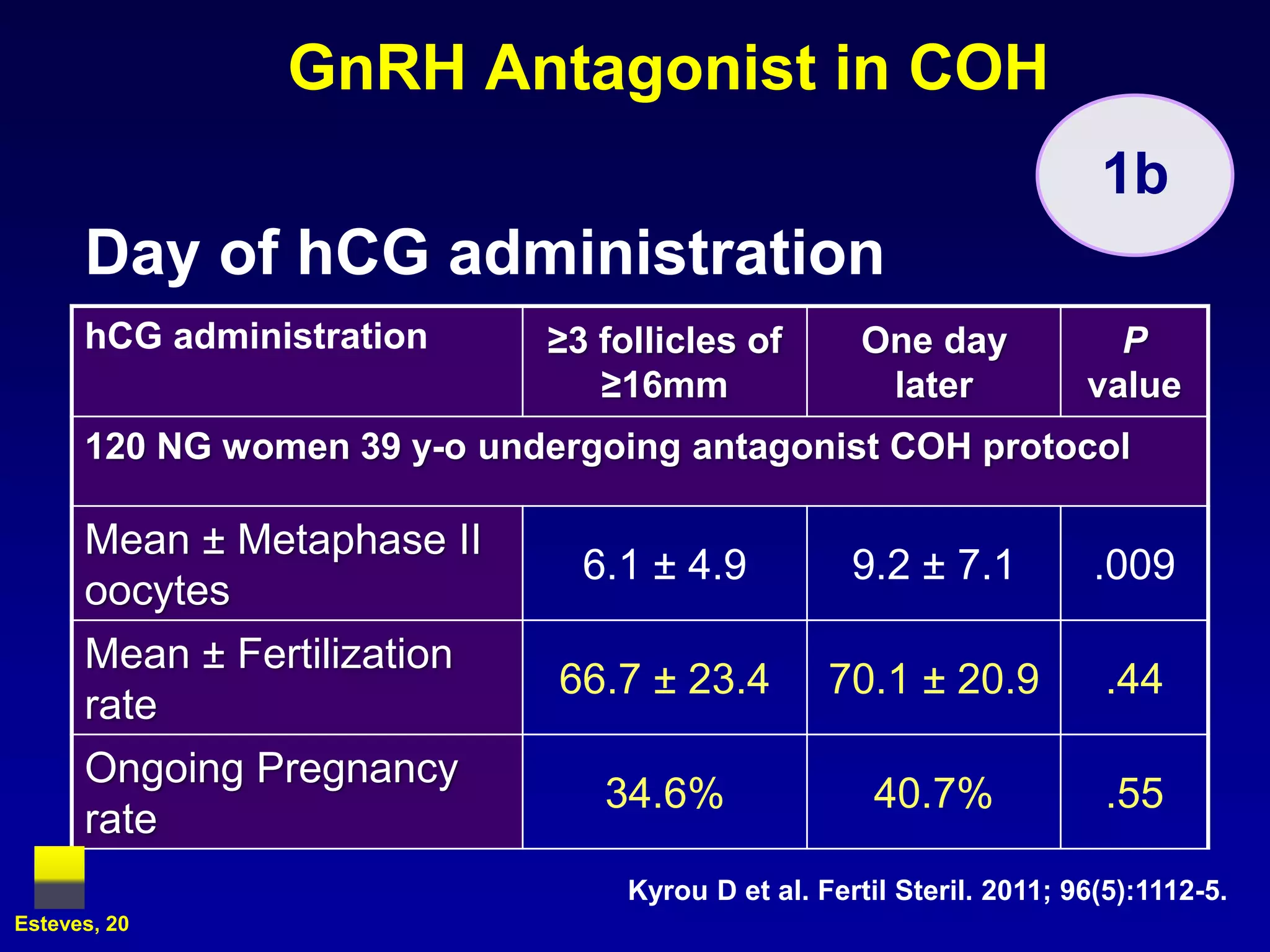
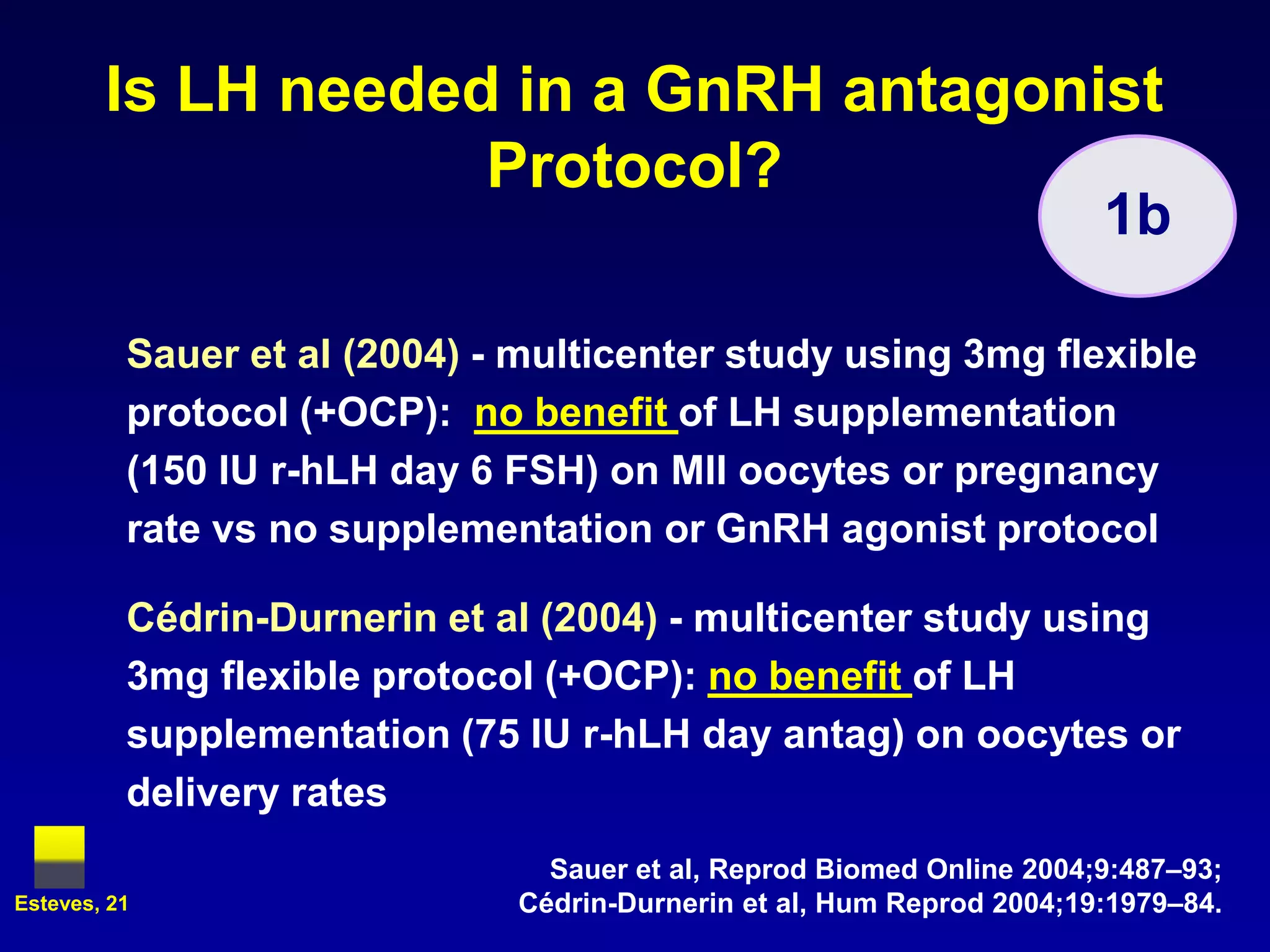
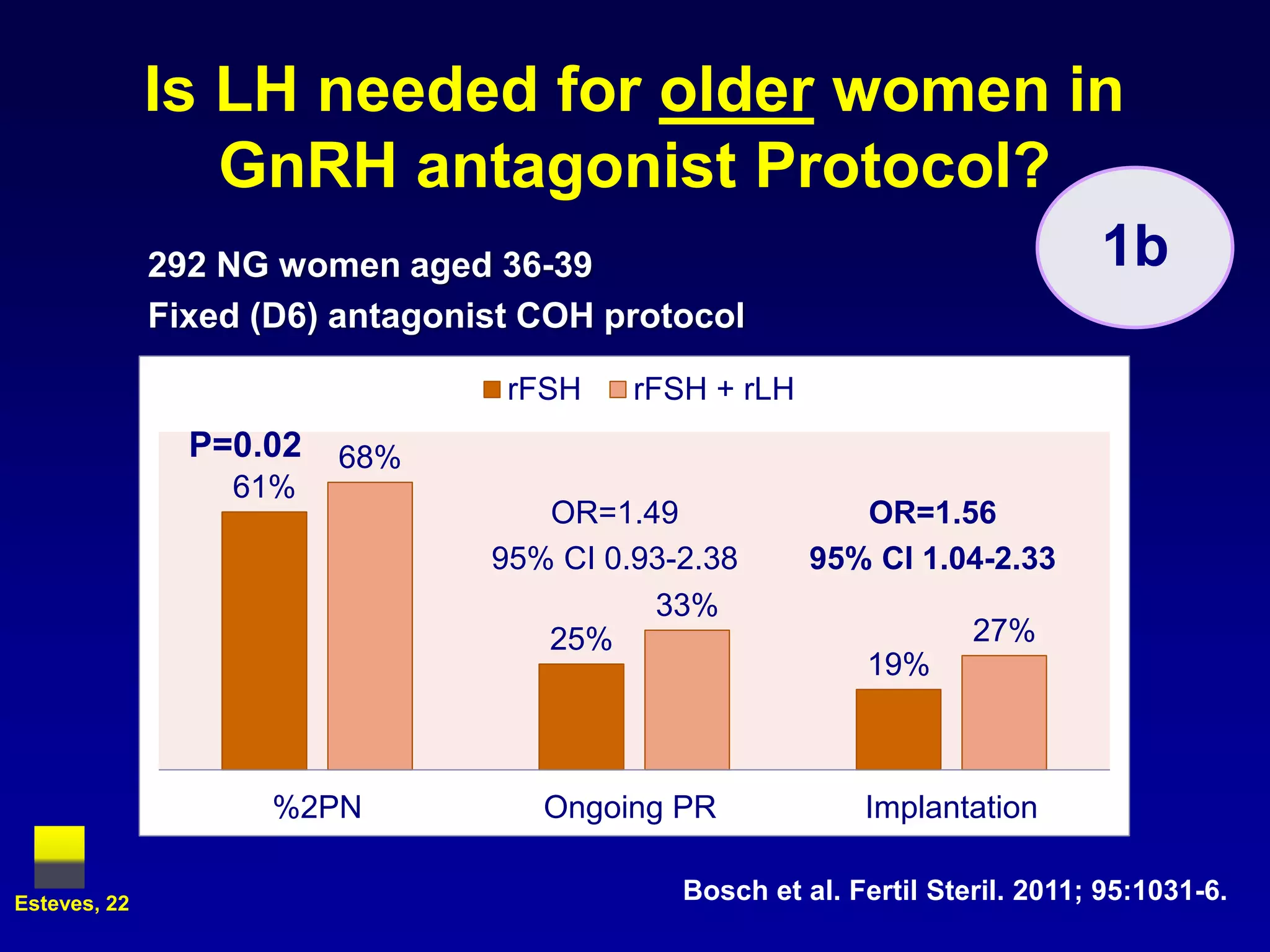
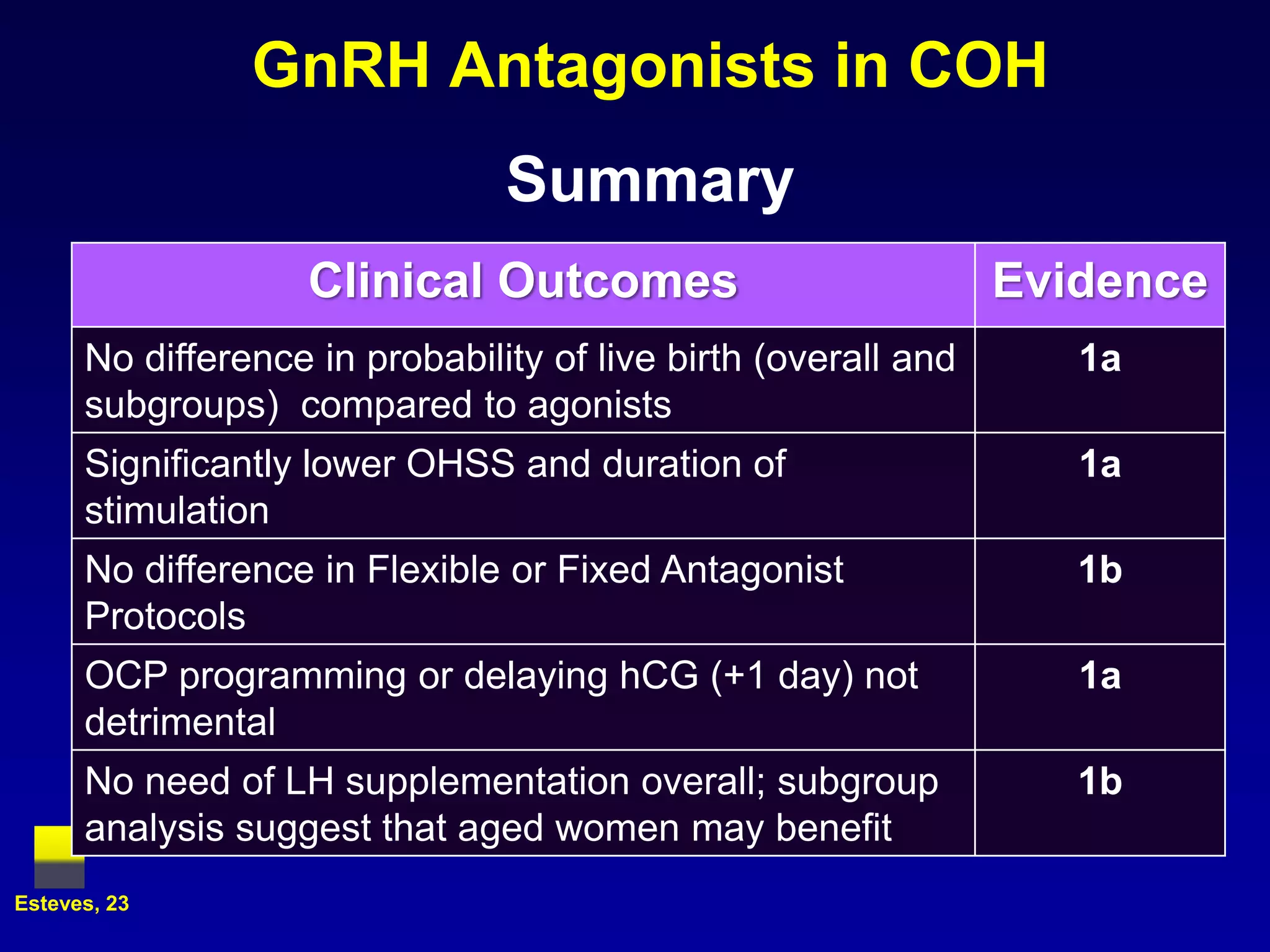
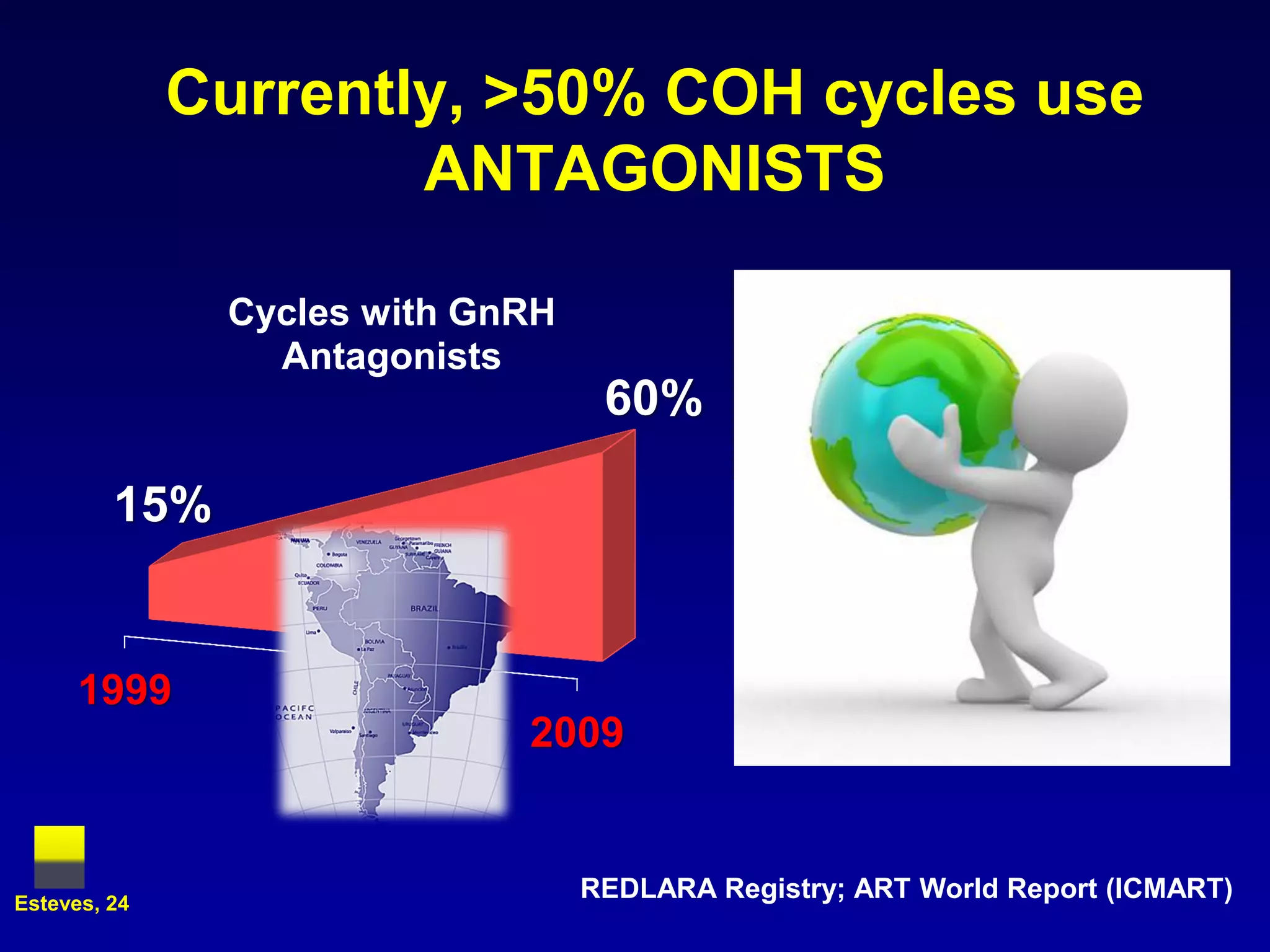
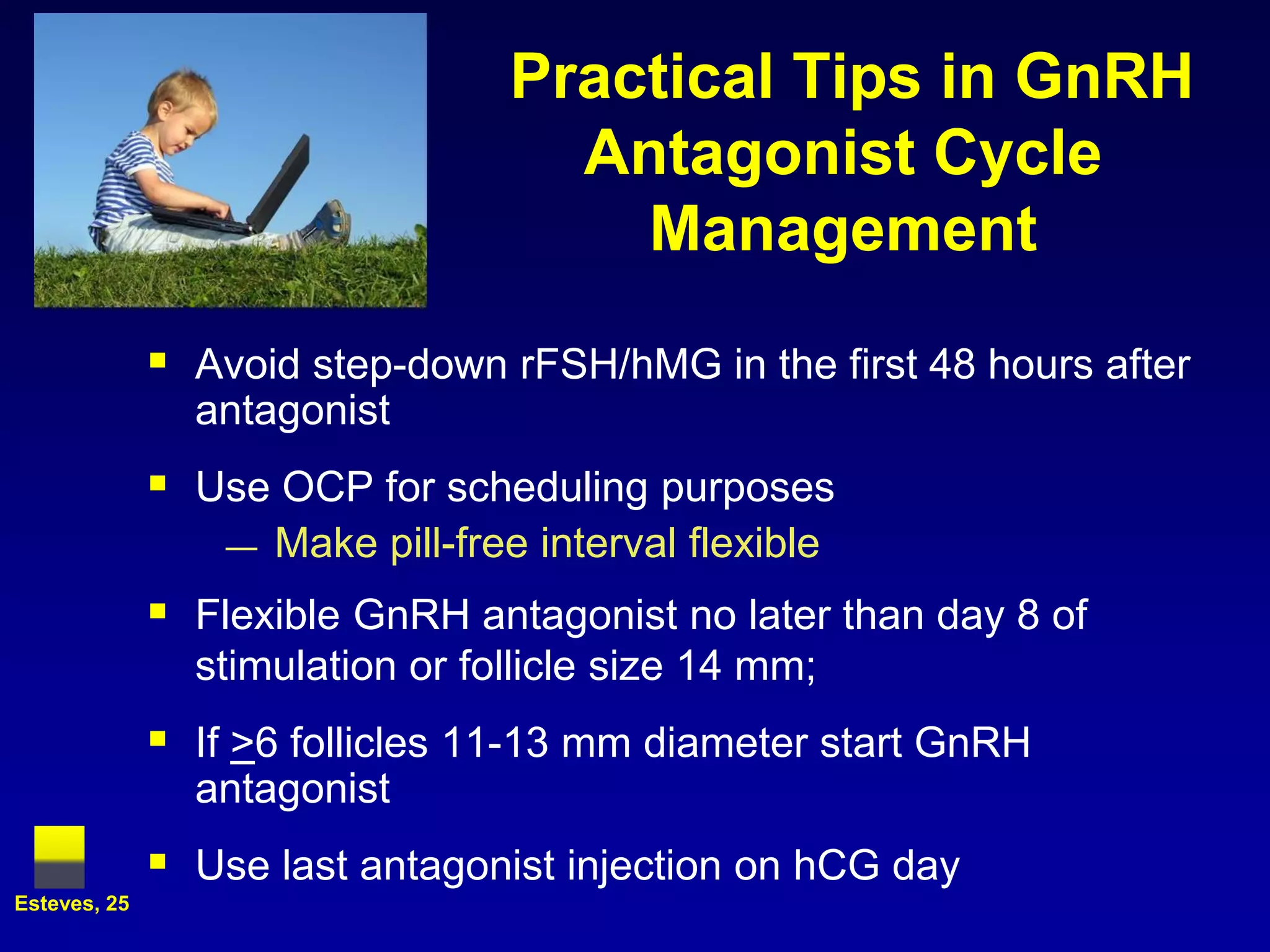

This document provides an overview of a lecture on LH suppression in controlled ovarian hyperstimulation (COH) using GnRH antagonists. The key points covered include: 1) The importance of LH suppression in COH to prevent premature luteinization and improve outcomes. 2) How GnRH antagonists can be used for LH suppression compared to agonists. Clinical trials show antagonists reduce OHSS risk and duration of stimulation compared to agonists without impacting live birth rates. 3) Flexible or fixed antagonist protocols, use of oral contraceptives, and timing of hCG administration do not significantly impact outcomes. LH supplementation is generally not needed.
































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









