Downloaded 13 times

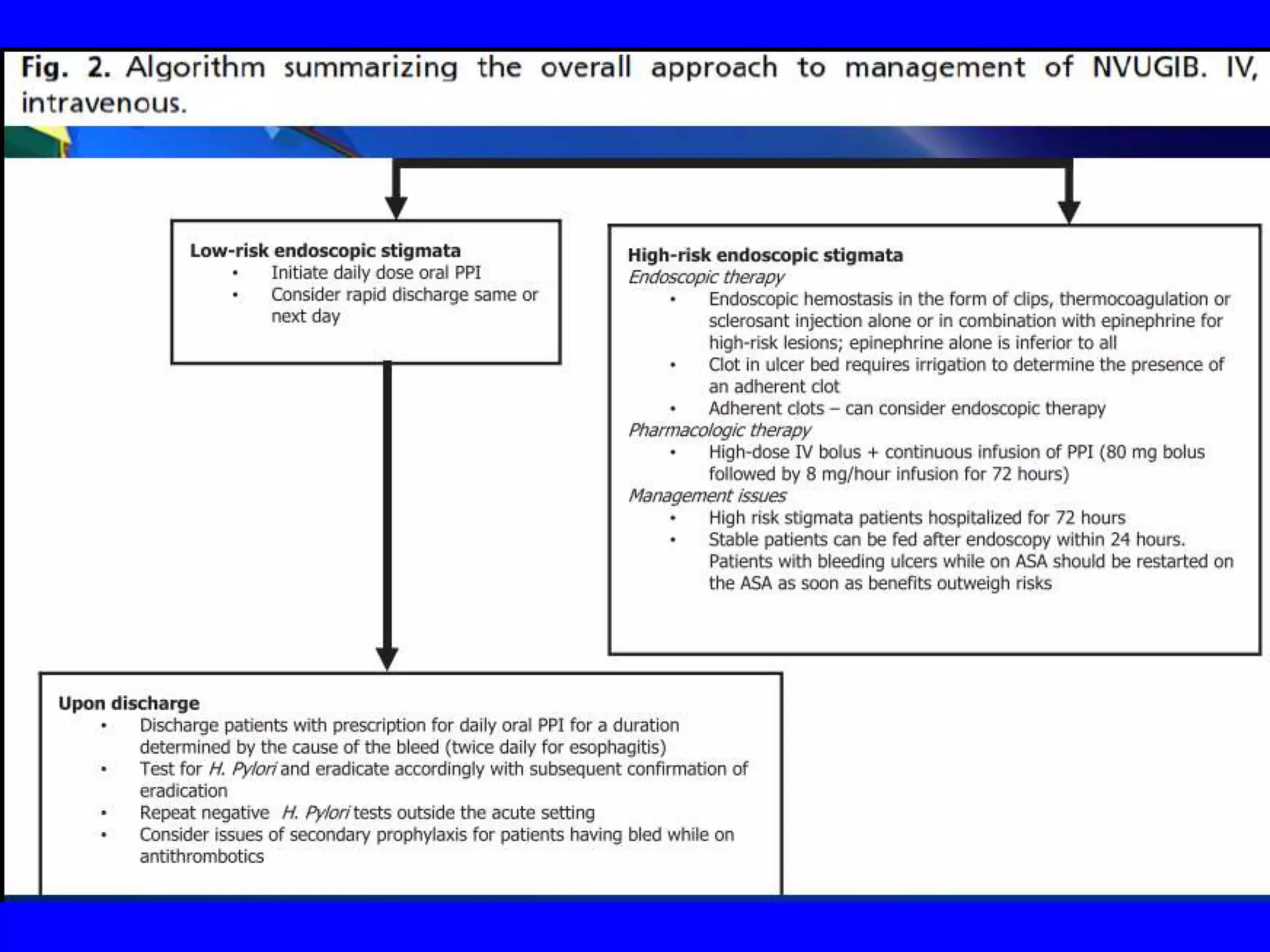
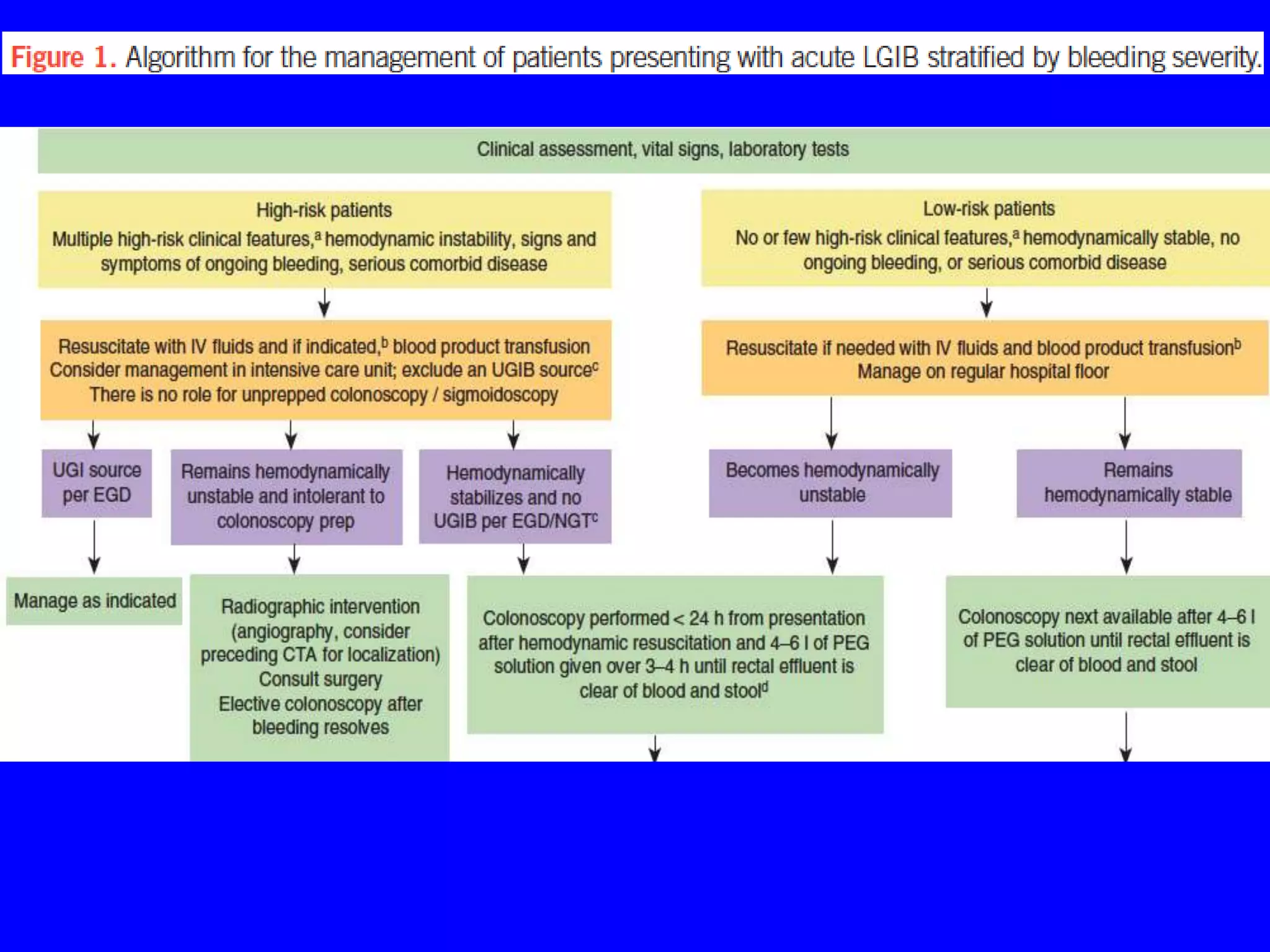
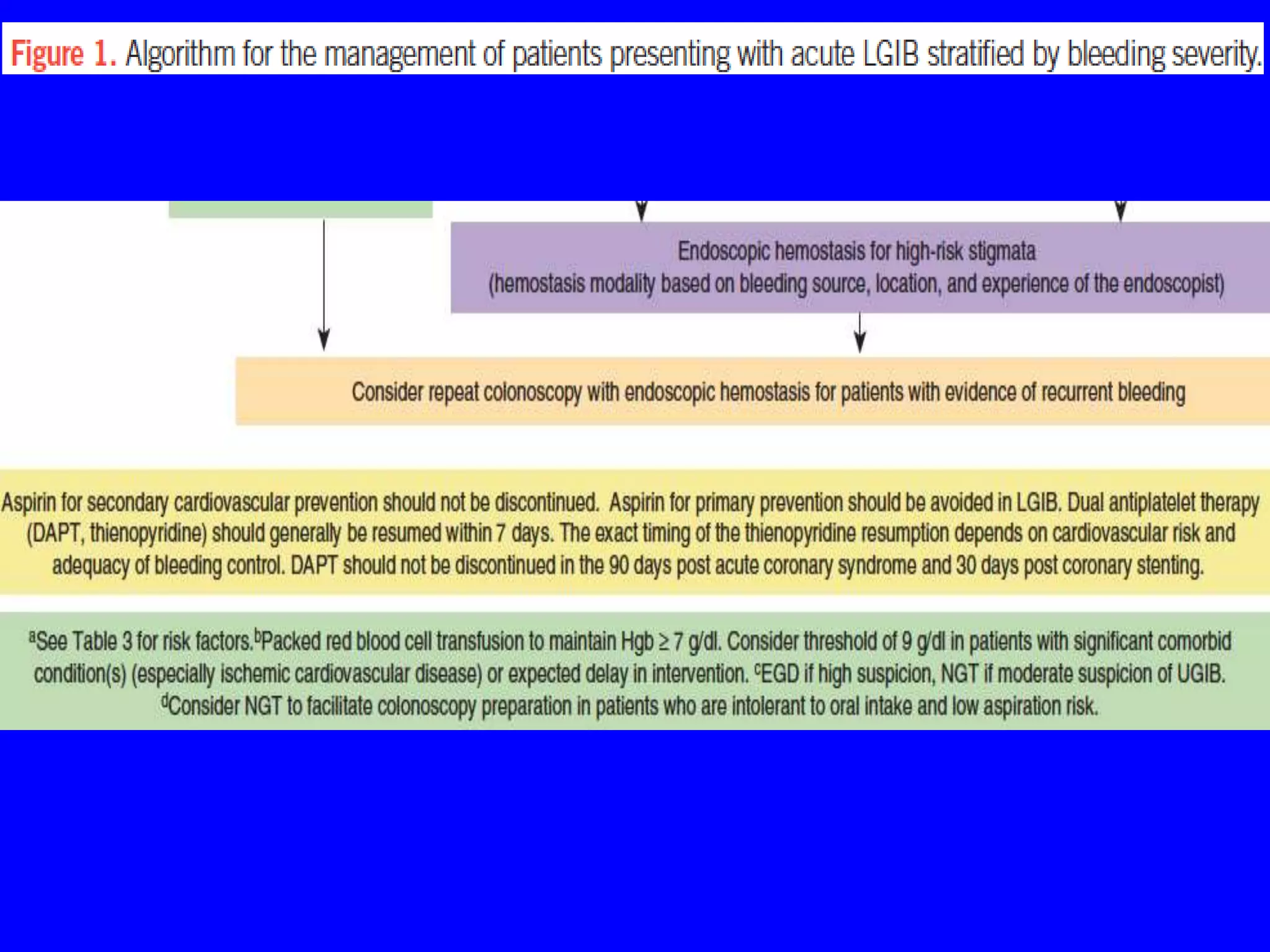
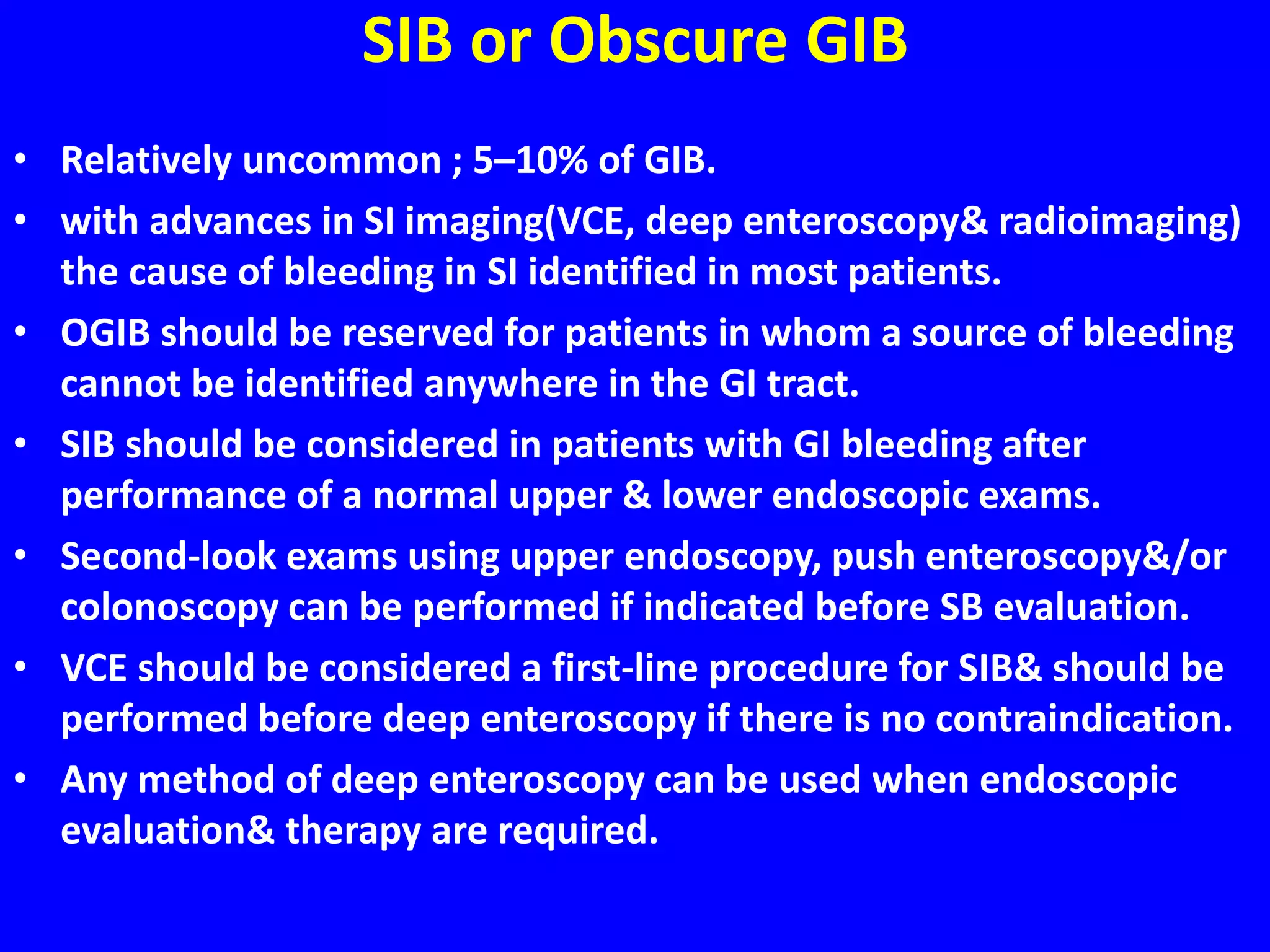
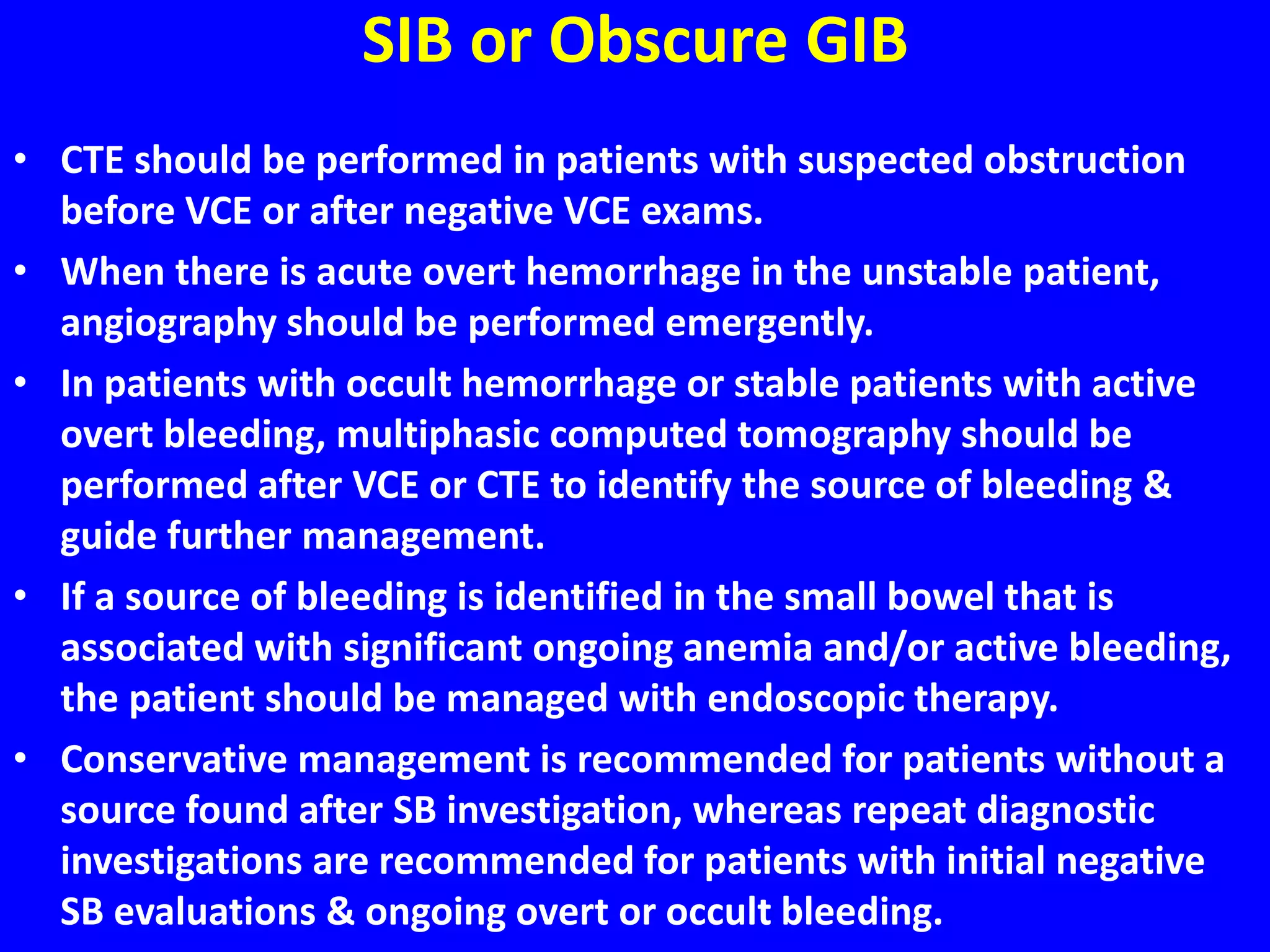


This document provides an overview of gastrointestinal bleeding (GIB), including the different types (upper, lower, small intestinal bleeding), typical causes, clinical presentations, evaluation, and management. Some key points: - Upper GIB is the most common type, accounting for 80% of cases, while small intestinal bleeding (SIB) is the least common at 5%. - The most common presentations of upper GIB are melena (black tarry stool) and hematemesis (vomiting blood), while hematochezia (fresh red blood per rectum) is more typical of lower GIB. - Evaluation involves assessing severity using scoring systems like the Glasgow-Blatchford score to determine


















































![GASTROINTESTINAL BLEED ARUP SIR [Autosaved] copy.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gastrointestinalbleed-arupsirautosavedcopy-250402060103-4e590a88-thumbnail.jpg?width=640&height=640&fit=bounds)
























































